

Global variations in funding and use of hemodialysis accesses: an international report using the ISN Global Kidney Health Atlas
- PMID: 38720263
- PMCID: PMC11080121
- DOI: 10.1186/s12882-024-03593-z
Global variations in funding and use of hemodialysis accesses: an international report using the ISN Global Kidney Health Atlas
Abstract
Background: There is a lack of contemporary data describing global variations in vascular access for hemodialysis (HD). We used the third iteration of the International Society of Nephrology Global Kidney Health Atlas (ISN-GKHA) to highlight differences in funding and availability of hemodialysis accesses used for initiating HD across world regions.
Methods: Survey questions were directed at understanding the funding modules for obtaining vascular access and types of accesses used to initiate dialysis. An electronic survey was sent to national and regional key stakeholders affiliated with the ISN between June and September 2022. Countries that participated in the survey were categorized based on World Bank Income Classification (low-, lower-middle, upper-middle, and high-income) and by their regional affiliation with the ISN.
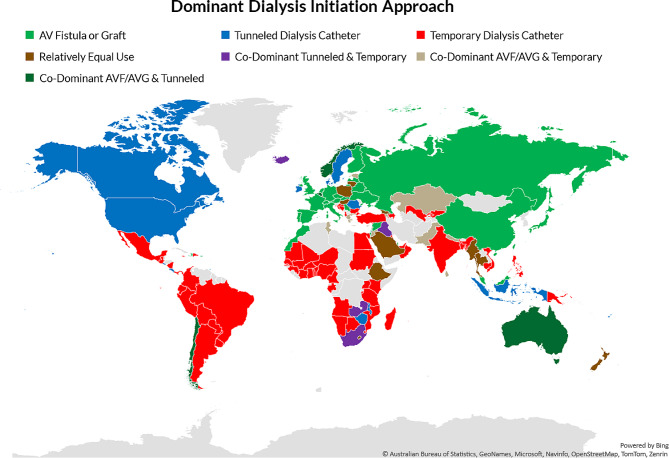
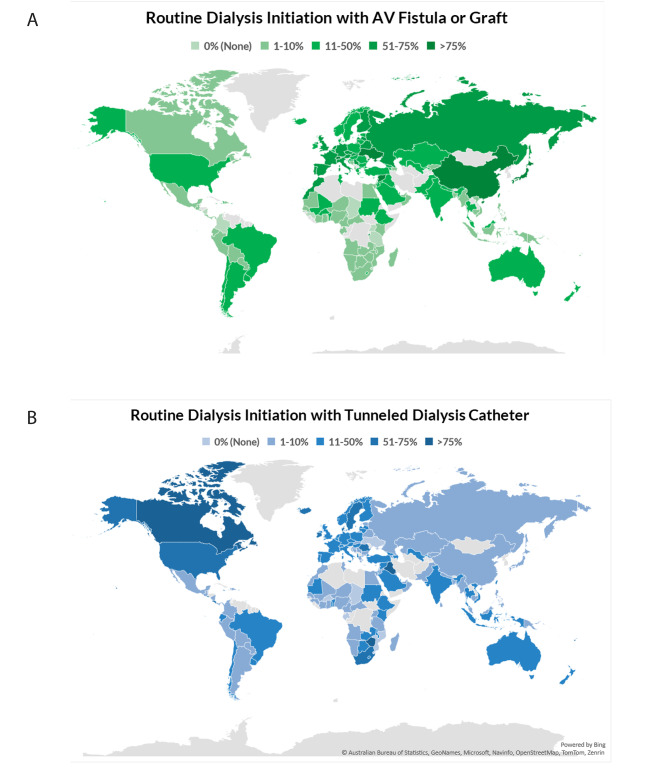
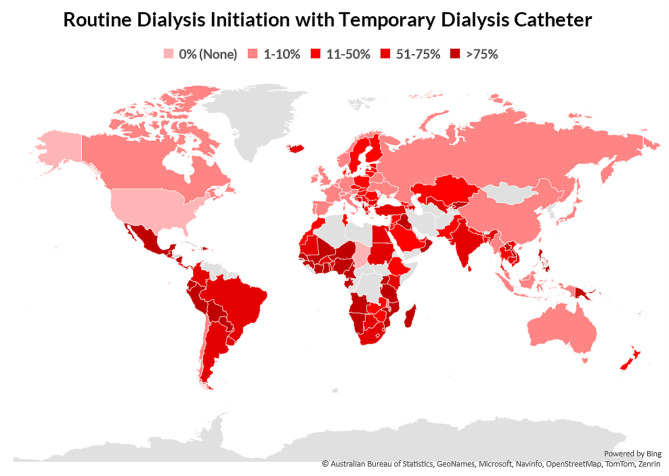
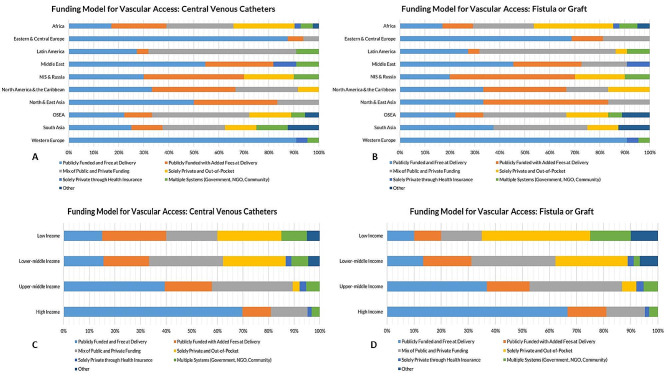
Results: Data on types of vascular access were available from 160 countries. Respondents from 35 countries (22% of surveyed countries) reported that > 50% of patients started HD with an arteriovenous fistula or graft (AVF or AVG). These rates were higher in Western Europe (n = 14; 64%), North & East Asia (n = 4; 67%), and among high-income countries (n = 24; 38%). The rates of > 50% of patients starting HD with a tunneled dialysis catheter were highest in North America & Caribbean region (n = 7; 58%) and lowest in South Asia and Newly Independent States and Russia (n = 0 in both regions). Respondents from 50% (n = 9) of low-income countries reported that > 75% of patients started HD using a temporary catheter, with the highest rates in Africa (n = 30; 75%) and Latin America (n = 14; 67%). Funding for the creation of vascular access was often through public funding and free at the point of delivery in high-income countries (n = 42; 67% for AVF/AVG, n = 44; 70% for central venous catheters). In low-income countries, private and out of pocket funding was reported as being more common (n = 8; 40% for AVF/AVG, n = 5; 25% for central venous catheters).
Conclusions: High income countries exhibit variation in the use of AVF/AVG and tunneled catheters. In low-income countries, there is a higher use of temporary dialysis catheters and private funding models for access creation.
Keywords: Arteriovenous fistulas; Central venous catheters; Dialysis; Global kidney Health Atlas; International Society of Nephrology; Kidney failure.
© 2024. The Author(s).
Conflict of interest statement
All authors have completed an ICMJE form. RK reports personal fees from Baxter healthcare, outside the submitted work. VAL reports royalties from Elsevier, consulting fees from the World Health Organization, travel support from the European Renal Association and International Society of Nephrology, and leadership role in Advocacy Working Group of the International Society of Nephrology, outside the submitted work. RRQ reports honoraria from Baxter Healthcare Corporation and the patent Dialysis Information Management System, Canada, outside the submitted work. NS reports personal fees from Baxter, grants and personal fees from Amgen, outside the submitted work. ST reports Fellowship grants from the International Society of Nephrology-Salmasi Family and the Kidney Foundation of Thailand, outside the submitted work. SA reports personal fees from The International Society of Nephrology, outside the submitted work. SD reports personal fees from The International Society of Nephrology, outside the submitted work. JD reports personal fees from The International Society of Nephrology, outside the submitted work. VJ reports personal fees from GSK, Astra Zeneca, Baxter Healthcare, Visterra, Biocryst, Chinook, Vera, and Bayer, paid to his institution, outside the submitted work. CM reports personal fees from The International Society of Nephrology, outside the submitted work. MN reports grants and personal fees from KyowaKirin, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Torii, JT, Mitsubishi Tanabe, grants from Takeda and Bayer, and personal fees from Astellas, Akebia, AstraZeneca, and GSK, outside the submitted work. AKB reports other (consultancy and honoraria) from AMGEN Incorporated and Otsuka, other (consultancy) from Bayer and GSK, and grants from Canadian Institute of Health Research and Heart and Stroke Foundation of Canada, outside the submitted work; He is also Associate Editor of the Canadian Journal of Kidney Health and Disease and Co-chair of the ISN-Global Kidney Health Atlas. DWJ reports consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer, and AWAK, speaker’s honoraria from ONO and Boehringer Ingelheim & Lilly, and travel sponsorships from Ono and Amgen, outside the submitted work. He is also a current recipient of an Australian National Health and Medical Research Council Leadership Investigator Grant, outside the submitted work. All other authors declare that they have no competing interests.
Figures
Similar articles
-
Global variability of vascular and peritoneal access for chronic dialysis.Nephrology (Carlton). 2024 Mar;29(3):135-142. doi: 10.1111/nep.14259. Epub 2023 Nov 29. Nephrology (Carlton). 2024. PMID: 38018697
-
Cost-effectiveness Analysis of Vascular Access Referral Policies in CKD.Am J Kidney Dis. 2017 Sep;70(3):368-376. doi: 10.1053/j.ajkd.2017.04.020. Epub 2017 Jun 7. Am J Kidney Dis. 2017. PMID: 28599902
-
Trends in US Vascular Access Use, Patient Preferences, and Related Practices: An Update From the US DOPPS Practice Monitor With International Comparisons.Am J Kidney Dis. 2015 Jun;65(6):905-15. doi: 10.1053/j.ajkd.2014.12.014. Epub 2015 Feb 7. Am J Kidney Dis. 2015. PMID: 25662834
-
Capacity for the management of kidney failure in the International Society of Nephrology Oceania and South East Asia (OSEA) region: report from the 2023 ISN Global Kidney Health Atlas (ISN-GKHA).Kidney Int Suppl (2011). 2024 Apr;13(1):110-122. doi: 10.1016/j.kisu.2024.01.004. Epub 2024 Apr 8. Kidney Int Suppl (2011). 2024. PMID: 38618497 Free PMC article. Review.
-
Capacity for the management of kidney failure in the International Society of Nephrology North and East Asia region: report from the 2023 ISN Global Kidney Health Atlas (ISN-GKHA).Kidney Int Suppl (2011). 2024 Apr;13(1):97-109. doi: 10.1016/j.kisu.2024.02.001. Epub 2024 Apr 8. Kidney Int Suppl (2011). 2024. PMID: 38618501 Free PMC article. Review.
Cited by
-
Prospective Analysis of Arteriovenous Fistula Performance in the Context of Competing Risks.Kidney360. 2025 Feb 1;6(2):272-283. doi: 10.34067/KID.0000000650. Epub 2024 Nov 19. Kidney360. 2025. PMID: 39560989 Free PMC article.
-
Registry of access to chronic dialysis initiation at the Public Health System in Brazil.Int Urol Nephrol. 2025 Jul 14. doi: 10.1007/s11255-025-04652-6. Online ahead of print. Int Urol Nephrol. 2025. PMID: 40660076
References
-
- Chan CT, Blankestijn PJ, Dember LM, Gallieni M, Harris DCH, Lok CE et al. Dialysis initiation, modality choice, access, and prescription: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;96(1):37–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
