

Effects of non-invasive respiratory support in post-operative patients: a systematic review and network meta-analysis
- PMID: 38720332
- PMCID: PMC11077852
- DOI: 10.1186/s13054-024-04924-0
Effects of non-invasive respiratory support in post-operative patients: a systematic review and network meta-analysis
Abstract
Background: Re-intubation secondary to post-extubation respiratory failure in post-operative patients is associated with increased patient morbidity and mortality. Non-invasive respiratory support (NRS) alternative to conventional oxygen therapy (COT), i.e., high-flow nasal oxygen, continuous positive airway pressure, and non-invasive ventilation (NIV), has been proposed to prevent or treat post-extubation respiratory failure. Aim of the present study is assessing the effects of NRS application, compared to COT, on the re-intubation rate (primary outcome), and time to re-intubation, incidence of nosocomial pneumonia, patient discomfort, intensive care unit (ICU) and hospital length of stay, and mortality (secondary outcomes) in adult patients extubated after surgery.
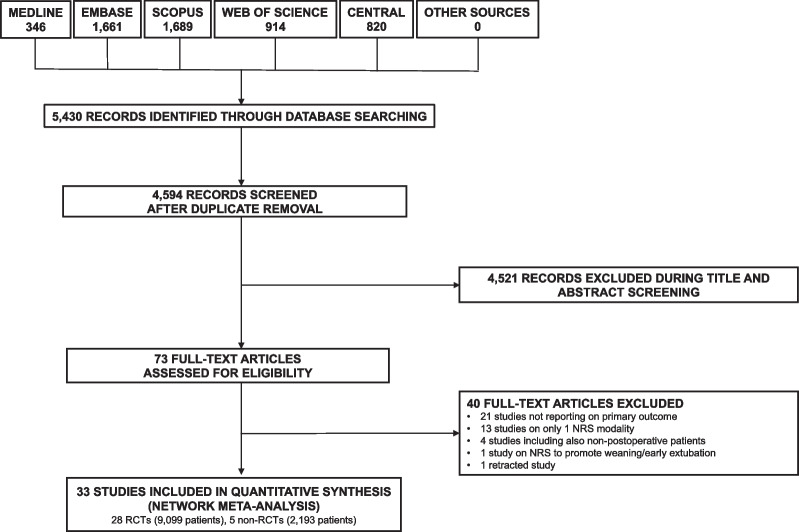
Methods: A systematic review and network meta-analysis of randomized and non-randomized controlled trials. A search from Medline, Embase, Scopus, Cochrane Central Register of Controlled Trials, and Web of Science from inception until February 2, 2024 was performed.
Results: Thirty-three studies (11,292 patients) were included. Among all NRS modalities, only NIV reduced the re-intubation rate, compared to COT (odds ratio 0.49, 95% confidence interval 0.28; 0.87, p = 0.015, I2 = 60.5%, low certainty of evidence). In particular, this effect was observed in patients receiving NIV for treatment, while not for prevention, of post-extubation respiratory failure, and in patients at high, while not low, risk of post-extubation respiratory failure. NIV reduced the rate of nosocomial pneumonia, ICU length of stay, and ICU, hospital, and long-term mortality, while not worsening patient discomfort.
Conclusions: In post-operative patients receiving NRS after extubation, NIV reduced the rate of re-intubation, compared to COT, when used for treatment of post-extubation respiratory failure and in patients at high risk of post-extubation respiratory failure.
Keywords: Continuous positive airway pressure; Conventional oxygen therapy; Extubation; General anesthesia; High-flow nasal oxygen; Non-invasive ventilation; Post-operative respiratory failure.
© 2024. The Author(s).
Conflict of interest statement
Prof. Navalesi’s research lab has received grants/research equipment from Draeger, Intersurgical SPA, and Gilead. Prof. Navalesi receives royalties from Intersurgical SPA for the Helmet Next invention. He has also received speaking fees from Getinge, Mindray, Intersurgical SPA, Gilead, GSK and Draeger. Dr. Zarantonello and Dr. Sella received payments for lecturing from Getinge. The other authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
