

Principles of surgery according to the Integral Theory Paradigm (ITP)
- PMID: 38721467
- PMCID: PMC11075963
- DOI: 10.21037/atm-23-1769
Principles of surgery according to the Integral Theory Paradigm (ITP)
Abstract
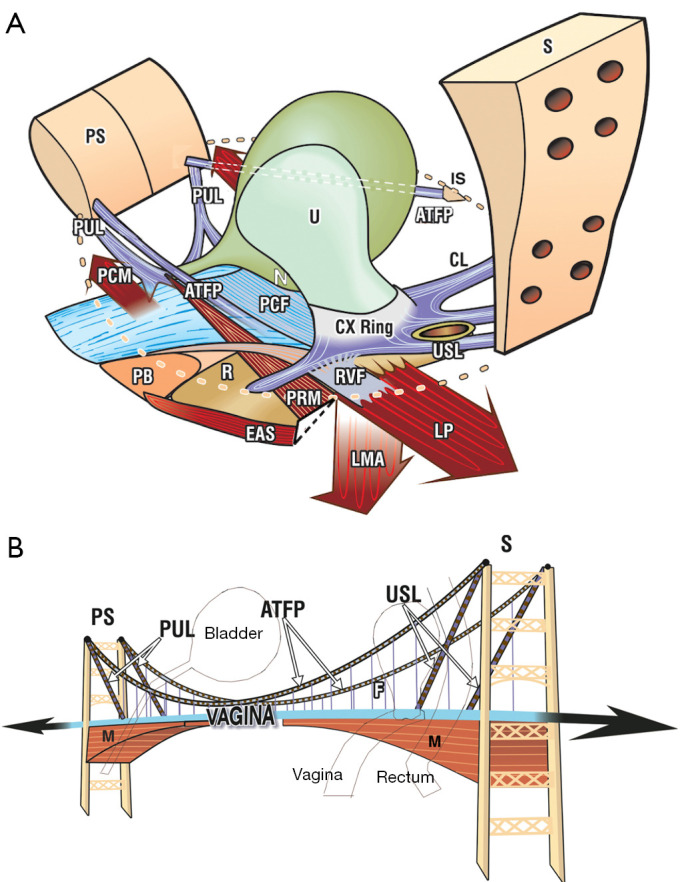
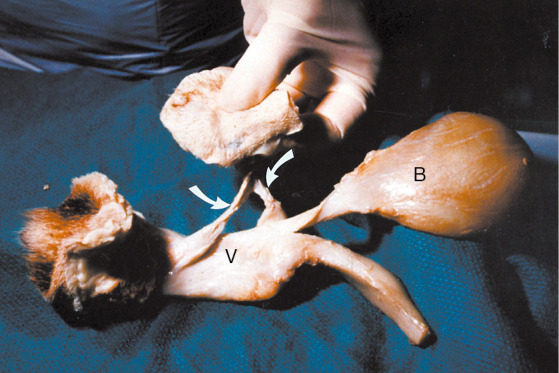
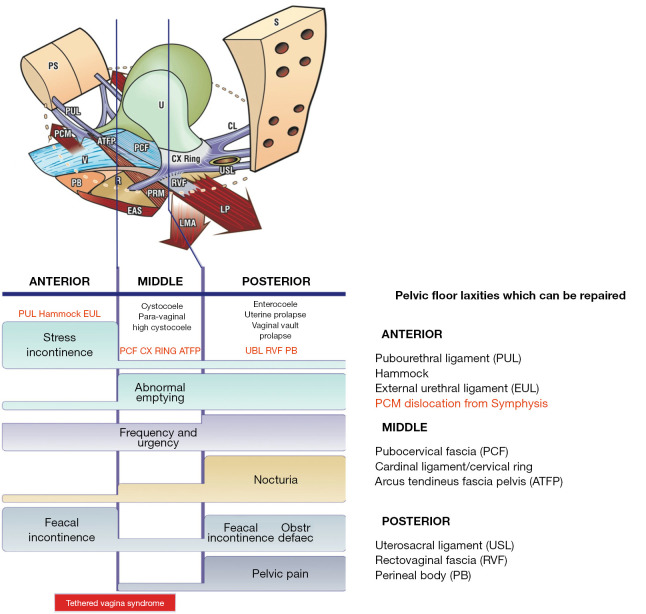
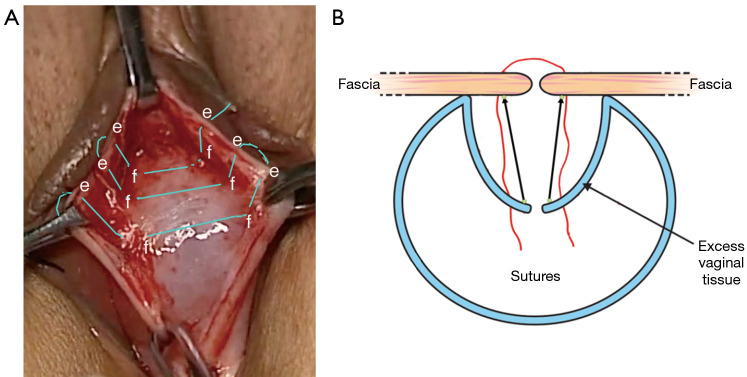
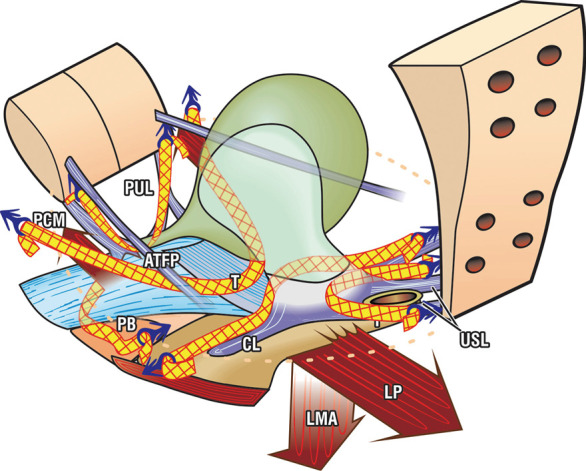
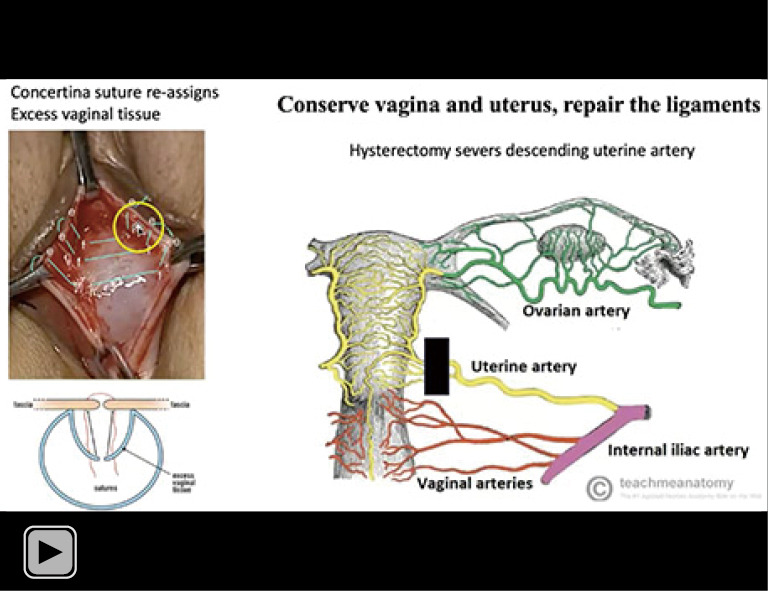
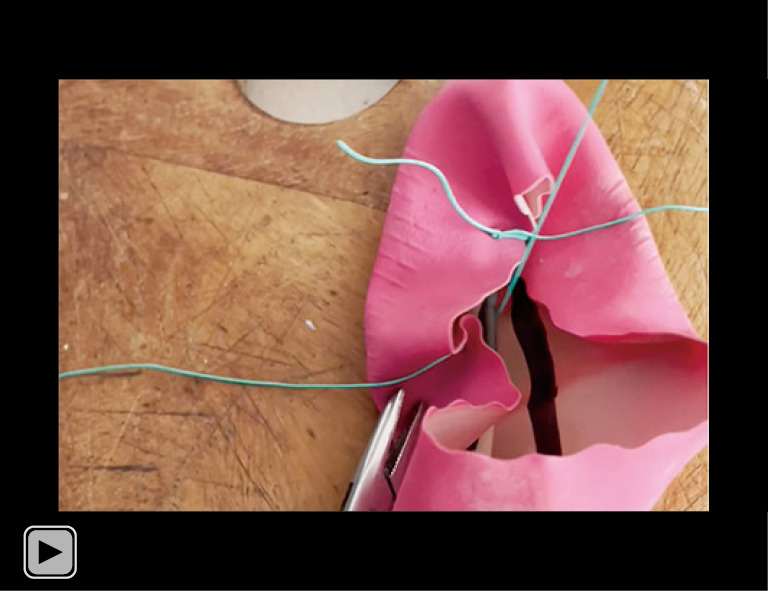
A core concept of the Integral Theory System is that "ligaments are for structure; vagina is for function". The vagina and uterus should be conserved. Because the vagina is an organ, its collagen and elastin, which are so necessary for its function, cannot regenerate once they are removed. Removing the uterus involves severing the descending uterine artery, which is the principal blood supply of the proximal part of the uterosacral ligaments (USLs), and so may cause atrophy, which can cause future incontinence problems because of collagen loss after menopause. The diagnostic algorithm guides which of the five pelvic ligaments need repair. Native ligament plication can be adequate for prolapse/symptom cure, but only in premenopausal women. Postmenopausal women are usually collagen deficient and require collagen-creating tapes or wide-bore polyester sutures to restore structural collagen in the ligaments. Of extreme importance, vaginal tissue excision should be avoided, as consequent scarring may cause "tethered vagina syndrome" (TVS). TVS can cause massive uncontrolled urine loss because the scar tissue in the bladder neck area of the vagina can link the more powerful posterior muscles to the anterior, so the posterior urethra wall is forcibly pulled open, when given the signal to close. Instead of vaginal excision, a "concertina" suture technique re-assigns and shrinks excess vaginal tissue to normal anatomy by 6 weeks. In conclusion, the five key surgical principles of the Integral Theory System are: ligaments are for structure, vagina is for function; structure (prolapse) and function (symptoms) are related; repair the structure and you will restore the function; avoid vaginal excision and hysterectomy; create new collagen to reinforce the damaged ligaments.
Keywords: Surgery principles; collagen; ligaments; polyester sutures; vagina.
2024 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-23-1769/coif). The series “Integral Theory Paradigm” was commissioned by the International Society for Pelviperineology without any funding or sponsorship. M.N. reports stocks and stock options at Momentis and Femselect. The authors have no other conflicts of interest to declare.
Figures
References
-
- An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet Gynecol Scand Suppl 1990;153:1-78. - PubMed
-
- Yamada H. Aging rate for the strength of human organs and tissues. In: Evans FG. editor. Strength of biological materials. Baltimore: Williams & Wilkins; 1970:272-80.
-
- Glazener CM, Breeman S, Elders A, et al. Mesh, graft, or standard repair for women having primary transvaginal anterior or posterior compartment prolapse surgery: two parallel-group, multicentre, randomised, controlled trials (PROSPECT). Lancet 2017;389:381-92. 10.1016/S0140-6736(16)31596-3 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources