

Electroencephalographic Correlates of Clinical Severity in the Natural history study of RTT and Related Disorders
- PMID: 38721759
- PMCID: PMC12045323
- DOI: 10.1002/ana.26948
Electroencephalographic Correlates of Clinical Severity in the Natural history study of RTT and Related Disorders
Abstract
Objective: This study was undertaken to characterize quantitative electroencephalographic (EEG) features in participants from the Natural history study of RTT and Related Disorders and to assess the potential for these features to act as objective measures of cortical function for Rett syndrome (RTT).
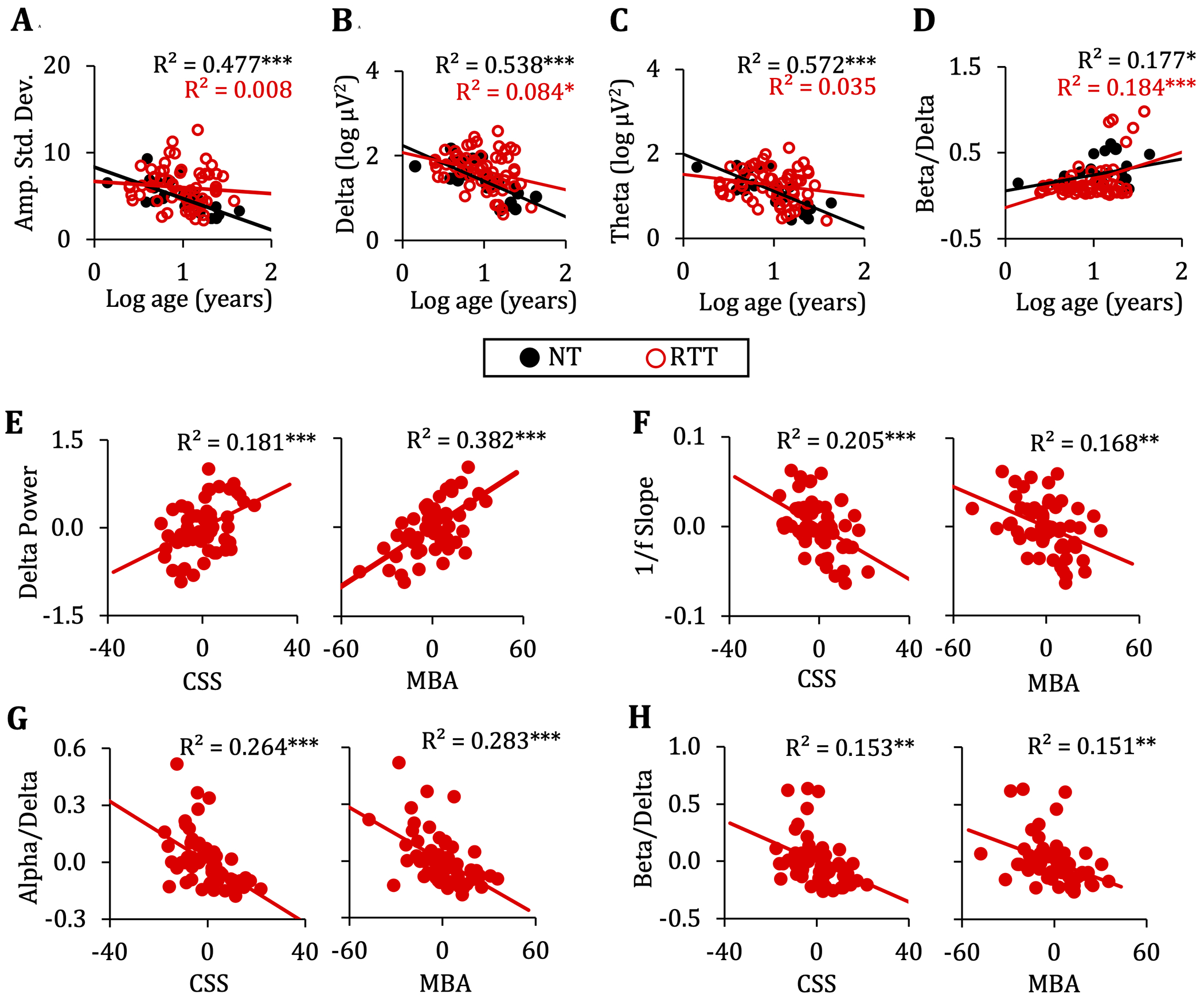
Methods: EEG amplitude and power features were derived from the resting EEG of 60 females with RTT (median age = 10.7 years) and 26 neurotypical females (median age = 10.6 years). Analyses focus on group differences and within the RTT group, associations between the EEG parameters and clinical severity. For a subset of participants (n = 20), follow-up data were available for assessing the reproducibility of the results and the stability in the parameters over 1 year.
Results: Compared to neurotypical participants, participants with RTT had greater amplitude variability and greater low-frequency activity as reflected by greater delta power, more negative 1/f slope, and lower theta/delta, alpha/delta, beta/delta, alpha/theta, and beta/theta ratios. Greater delta power, more negative 1/f slope, and lower power ratios were associated with greater severity. Analyses of year 1 data replicated the associations between 1/f slope and power ratios and clinical severity and demonstrated good within-subject consistency in these measures.
Interpretation: Overall, group comparisons reflected a greater predominance of lower versus higher frequency activity in participants with RTT, which is consistent with prior clinical interpretations of resting EEG in this population. The observed associations between the EEG power measures and clinical assessments and the repeatability of these measures underscore the potential for EEG to provide an objective measure of cortical function and clinical severity for RTT. ANN NEUROL 2024;96:175-186.
© 2024 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
Nothing to report.
Figures





References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
