

Impacts of environmental factors on the aetiological diagnosis and disease severity of community-acquired pneumonia in China: a multicentre, hospital-based, observational study
- PMID: 38721832
- PMCID: PMC11131030
- DOI: 10.1017/S0950268824000700
Impacts of environmental factors on the aetiological diagnosis and disease severity of community-acquired pneumonia in China: a multicentre, hospital-based, observational study
Abstract
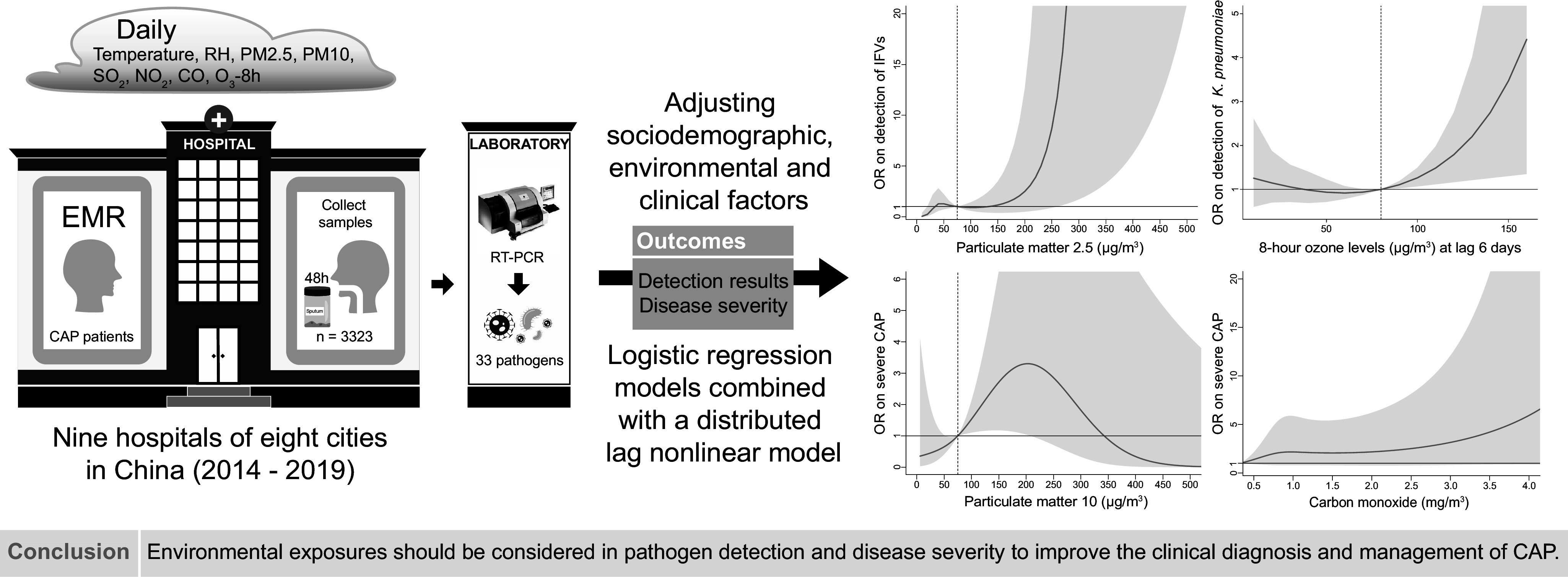
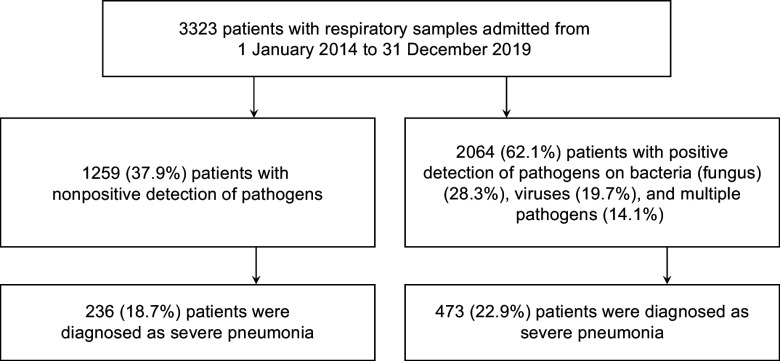
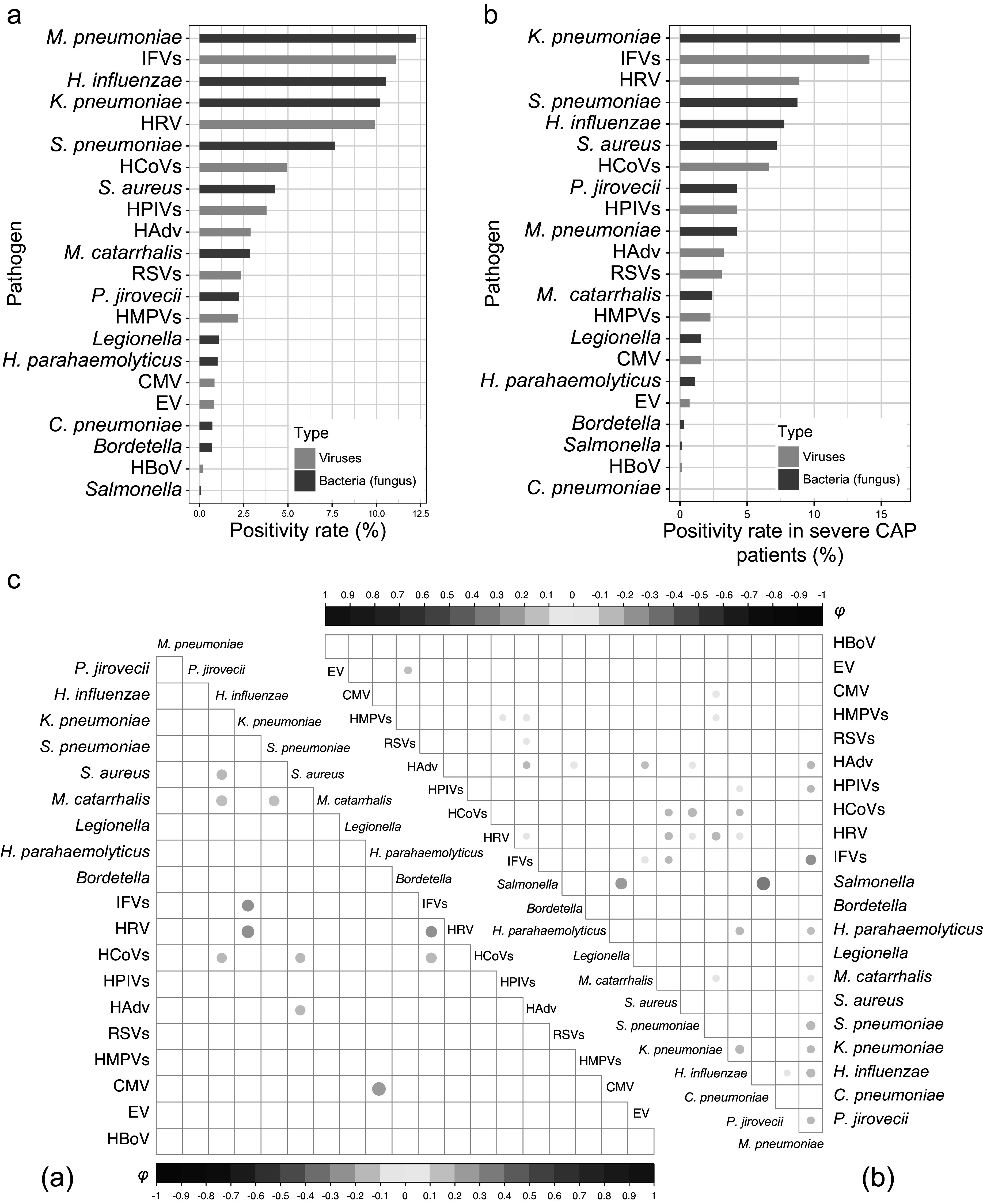
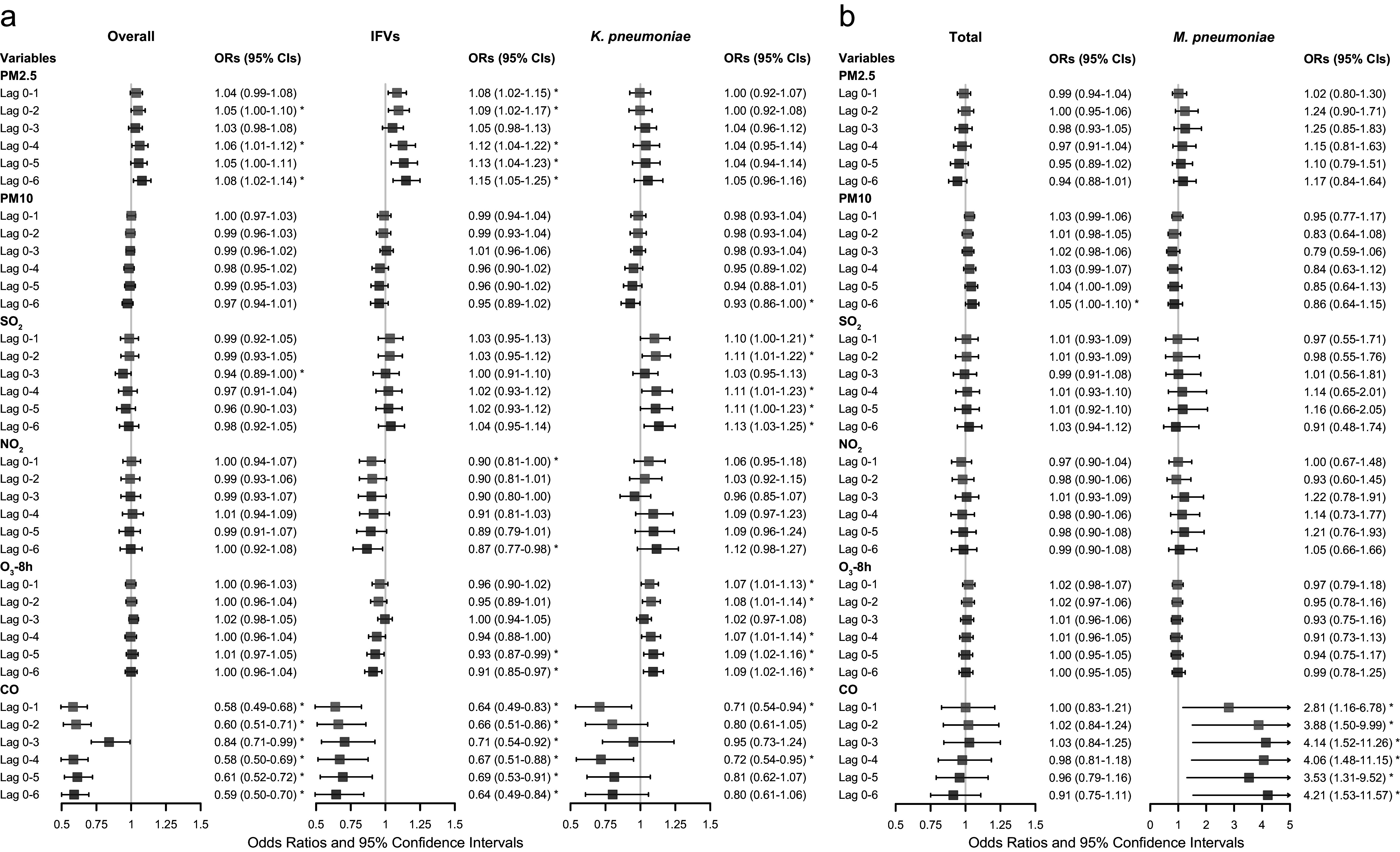
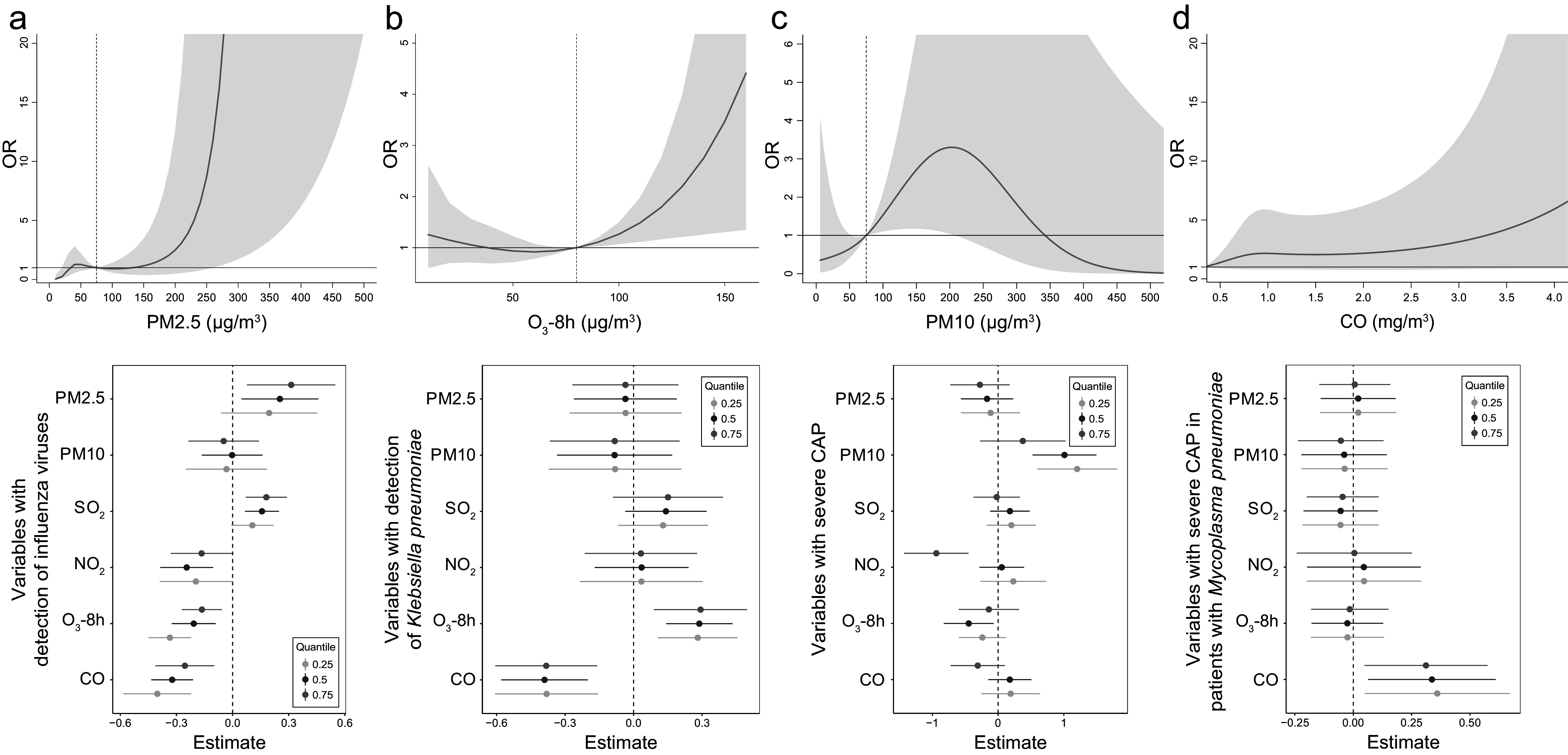
Environmental exposures are known to be associated with pathogen transmission and immune impairment, but the association of exposures with aetiology and severity of community-acquired pneumonia (CAP) are unclear. A retrospective observational study was conducted at nine hospitals in eight provinces in China from 2014 to 2019. CAP patients were recruited according to inclusion criteria, and respiratory samples were screened for 33 respiratory pathogens using molecular test methods. Sociodemographic, environmental and clinical factors were used to analyze the association with pathogen detection and disease severity by logistic regression models combined with distributed lag nonlinear models. A total of 3323 CAP patients were included, with 709 (21.3%) having severe illness. 2064 (62.1%) patients were positive for at least one pathogen. More severe patients were found in positive group. After adjusting for confounders, particulate matter (PM) 2.5 and 8-h ozone (O3-8h) were significant association at specific lag periods with detection of influenza viruses and Klebsiella pneumoniae respectively. PM10 and carbon monoxide (CO) showed cumulative effect with severe CAP. Pollutants exposures, especially PM, O3-8h, and CO should be considered in pathogen detection and severity of CAP to improve the clinical aetiological and disease severity diagnosis.
Keywords: aetiology; community-acquired pneumonia; disease severity; environmental factors; respiratory pathogens.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
