

Association between physician age and patterns of end-of-life care among older Americans
- PMID: 38721884
- PMCID: PMC11226372
- DOI: 10.1111/jgs.18939
Association between physician age and patterns of end-of-life care among older Americans
Abstract
Background: End-of-life (EOL) care patterns may differ by physician age given differences in how physicians are trained or changes associated with aging. We sought to compare patterns of EOL care delivered to older Americans according to physician age.
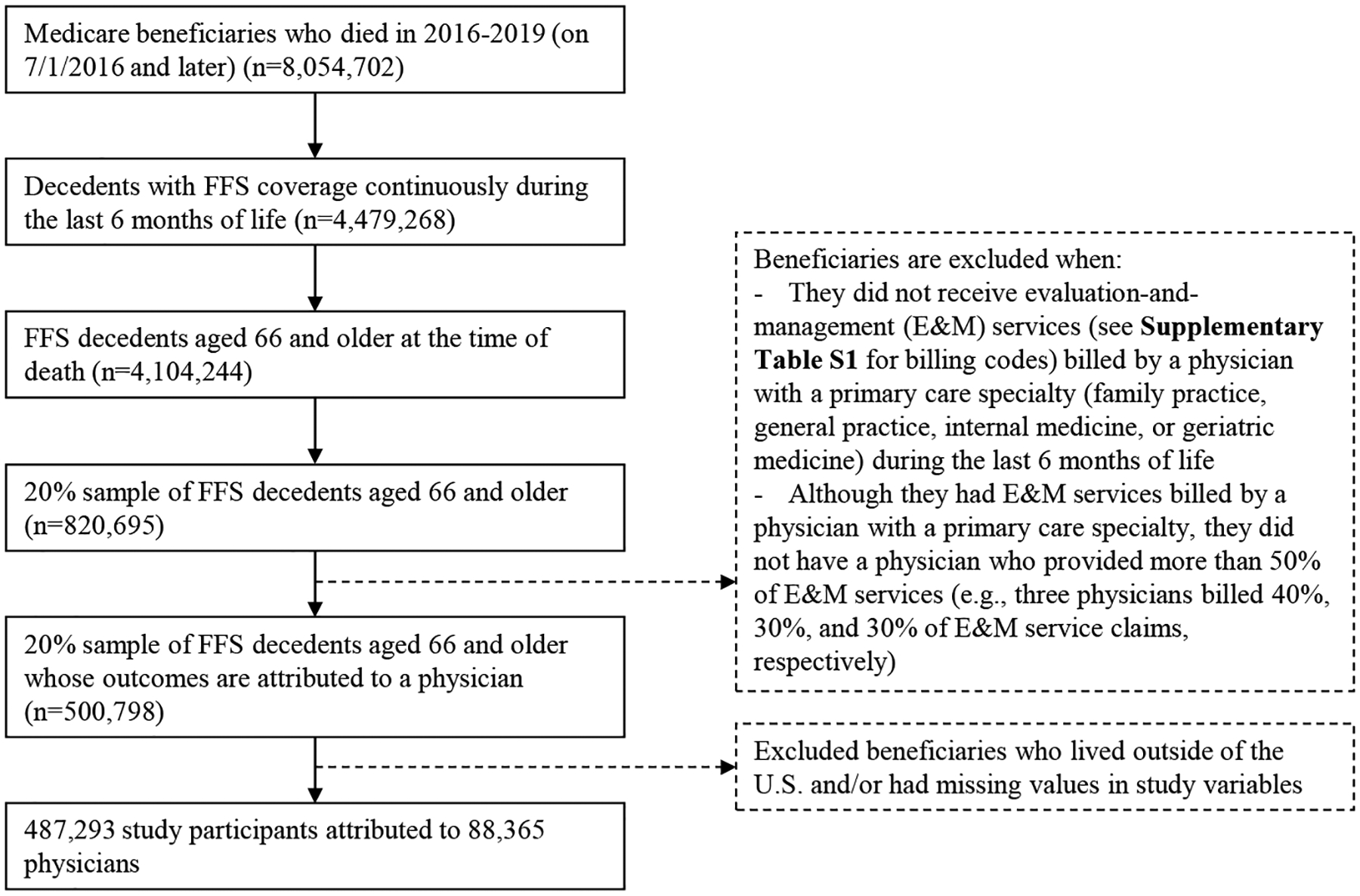
Methods: We conducted a cross-sectional study of a 20% sample of Medicare fee-for-service beneficiaries aged ≥66 years who died in 2016-2019 (n = 487,293). We attributed beneficiaries to the physician who had >50% of primary care visits during the last 6 months of life. We compared beneficiary-level outcomes by physician age (<40, 40-49, 50-59, or ≥60) in two areas: (1) advance care planning (ACP) and palliative care; and (2) high-intensity care at the EOL.
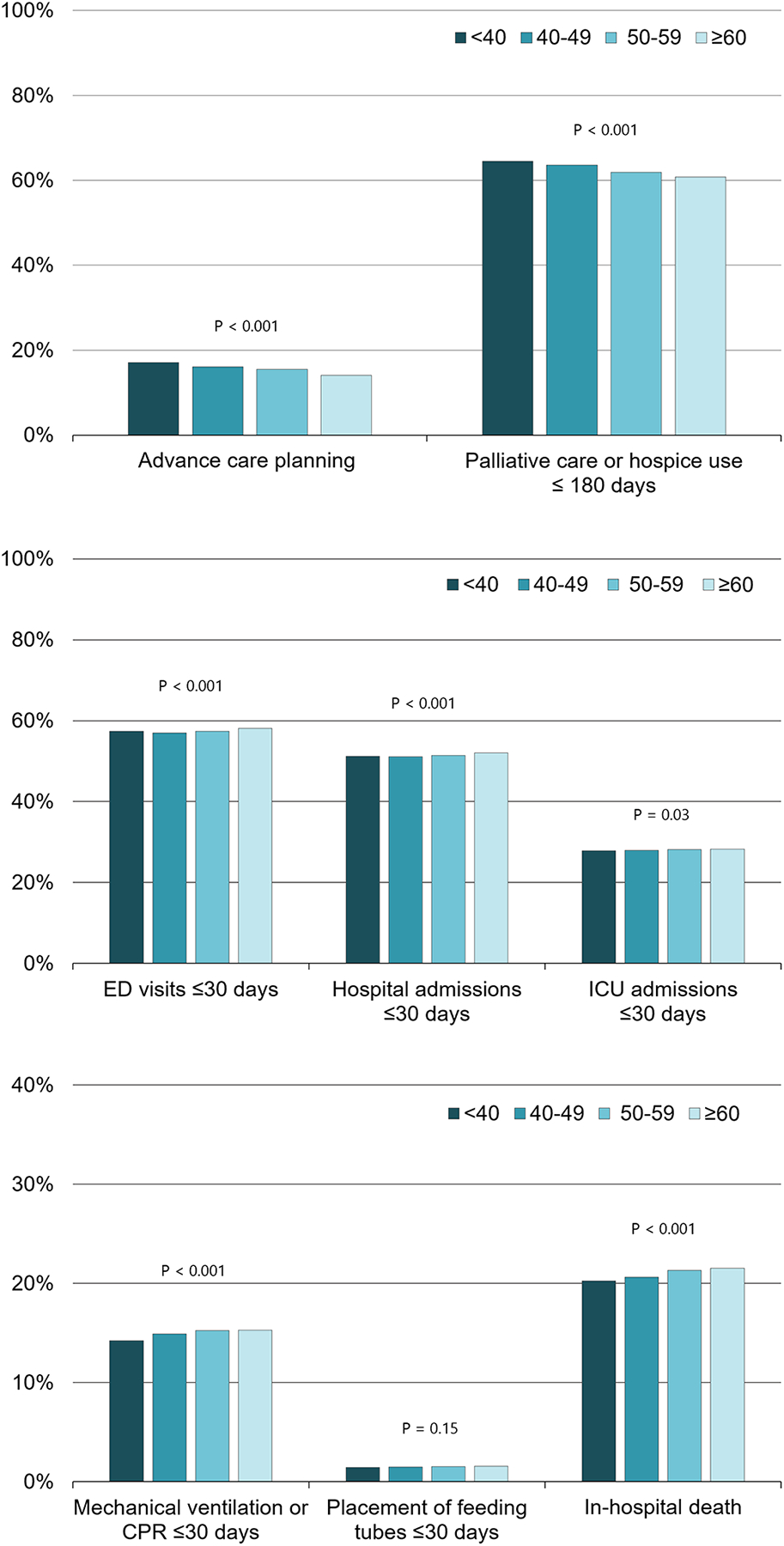
Results: Beneficiaries attributed to younger physicians had slightly higher proportions of billed ACP (adjusted proportions, 17.1%, 16.1%, 15.5%, and 14.0% for physicians aged <40, 40-49, 50-59, and ≥60, respectively; p-for-trend adjusted for multiple comparisons <0.001) and palliative care counseling or hospice use in the last 180 days of life (64.5%, 63.6%, 61.9%, and 60.8%; p-for-trend <0.001). Similarly, physicians' younger age was associated with slightly lower proportions of emergency department visits (57.4%, 57.0%, 57.4%, and 58.1%; p-for-trend <0.001), hospital admissions (51.2%, 51.1%, 51.4%, and 52.1%; p-for-trend <0.001), intensive care unit admissions (27.8%, 27.9%, 28.2%, and 28.3%; p-for-trend = 0.03), or mechanical ventilation or cardiopulmonary resuscitation (14.2, 14.9%, 15.2%, and 15.3%; p-for-trend <0.001) in the last 30 days of life, and in-hospital death (20.2%, 20.6%, 21.3%, and 21.5%; p-for-trend <0.001).
Conclusions: We found that differences in patterns of EOL care between beneficiaries cared for by younger and older physicians were small, and thus, not clinically meaningful. Future research is warranted to understand the factors that can influence patterns of EOL care provided by physicians, including initial and continuing medical education.
Keywords: advance care planning; end‐of‐life care; palliative care; physician age.
© 2024 The American Geriatrics Society.
Conflict of interest statement
Conflict of Interest Disclosures:
Dr. Jena reports receiving (in the last 36 months) consulting fees unrelated to this work from Bioverativ, Merck/Sharp/Dohme, Janssen, Edwards Life Sciences, Amgen, Eisai, Otsuka Pharmaceuticals, Vertex Pharmaceuticals, Sage Therapeutics, and Analysis Group. Dr. Jena also reports receiving (in the last 36 months) income unrelated to this work from hosting the podcast Freakonomics, M.D., from book rights to Doubleday Books, and from speaking fees from AAE and the Harry Walker Agency.
Figures
References
-
- Chodosh J, Mittman BS, Connor KI, et al. Caring for patients with dementia: how good is the quality of care? Results from three health systems. J Am Geriatr Soc. 2007;55(8):1260–1268. - PubMed
-
- Wenger NS, Roth CP, Martin D, et al. Quality of care provided in a special needs plan using a nurse care manager model. J Am Geriatr Soc 2011;59(10):1810–1822. - PubMed
-
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life. Washington (DC): National Academies Press (US); 2015. - PubMed
