

Implementable Prediction of Pressure Injuries in Hospitalized Adults: Model Development and Validation
- PMID: 38722209
- PMCID: PMC11094428
- DOI: 10.2196/51842
Implementable Prediction of Pressure Injuries in Hospitalized Adults: Model Development and Validation
Abstract
Background: Numerous pressure injury prediction models have been developed using electronic health record data, yet hospital-acquired pressure injuries (HAPIs) are increasing, which demonstrates the critical challenge of implementing these models in routine care.
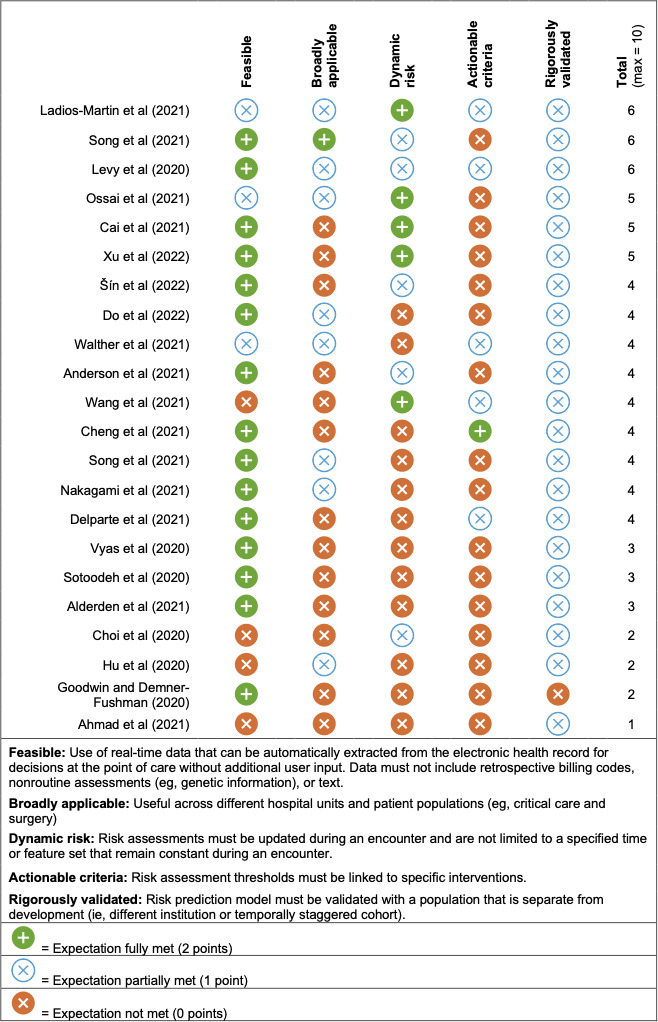
Objective: To help bridge the gap between development and implementation, we sought to create a model that was feasible, broadly applicable, dynamic, actionable, and rigorously validated and then compare its performance to usual care (ie, the Braden scale).
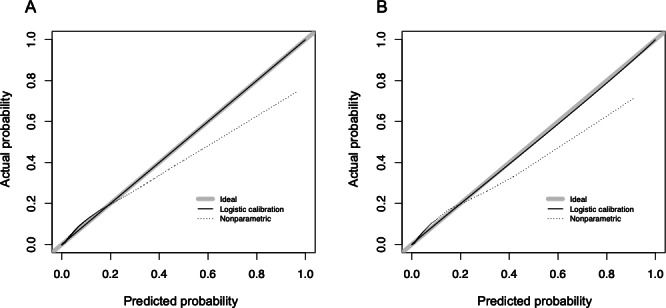
Methods: We extracted electronic health record data from 197,991 adult hospital admissions with 51 candidate features. For risk prediction and feature selection, we used logistic regression with a least absolute shrinkage and selection operator (LASSO) approach. To compare the model with usual care, we used the area under the receiver operating curve (AUC), Brier score, slope, intercept, and integrated calibration index. The model was validated using a temporally staggered cohort.
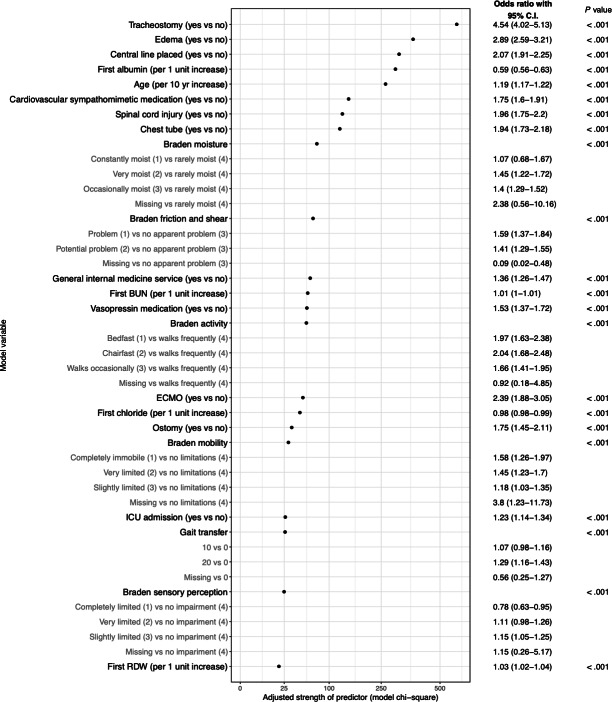
Results: A total of 5458 HAPIs were identified between January 2018 and July 2022. We determined 22 features were necessary to achieve a parsimonious and highly accurate model. The top 5 features included tracheostomy, edema, central line, first albumin measure, and age. Our model achieved higher discrimination than the Braden scale (AUC 0.897, 95% CI 0.893-0.901 vs AUC 0.798, 95% CI 0.791-0.803).
Conclusions: We developed and validated an accurate prediction model for HAPIs that surpassed the standard-of-care risk assessment and fulfilled necessary elements for implementation. Future work includes a pragmatic randomized trial to assess whether our model improves patient outcomes.
Keywords: EHR; adult; development; electronic health record; hospitalization; implementation; injury; patient safety; prediction; prediction model; predictive analytics; pressure injury; pressure sore; routine care.
© Thomas J Reese, Henry J Domenico, Antonio Hernandez, Daniel W Byrne, Ryan P Moore, Jessica B Williams, Brian J Douthit, Elise Russo, Allison B McCoy, Catherine H Ivory, Bryan D Steitz, Adam Wright. Originally published in JMIR Medical Informatics (https://medinform.jmir.org).
Conflict of interest statement
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
