

Natural language processing augments comorbidity documentation in neurosurgical inpatient admissions
- PMID: 38723044
- PMCID: PMC11081267
- DOI: 10.1371/journal.pone.0303519
Natural language processing augments comorbidity documentation in neurosurgical inpatient admissions
Abstract
Objective: To establish whether or not a natural language processing technique could identify two common inpatient neurosurgical comorbidities using only text reports of inpatient head imaging.
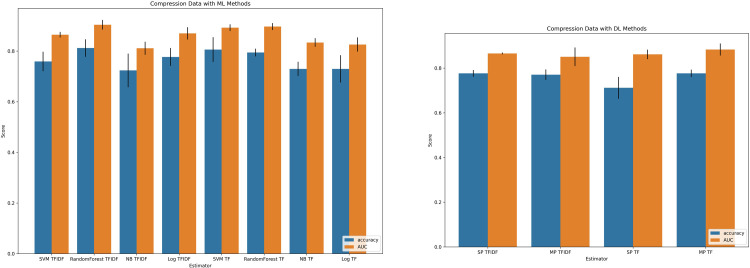
Materials and methods: A training and testing dataset of reports of 979 CT or MRI scans of the brain for patients admitted to the neurosurgery service of a single hospital in June 2021 or to the Emergency Department between July 1-8, 2021, was identified. A variety of machine learning and deep learning algorithms utilizing natural language processing were trained on the training set (84% of the total cohort) and tested on the remaining images. A subset comparison cohort (n = 76) was then assessed to compare output of the best algorithm against real-life inpatient documentation.
Results: For "brain compression", a random forest classifier outperformed other candidate algorithms with an accuracy of 0.81 and area under the curve of 0.90 in the testing dataset. For "brain edema", a random forest classifier again outperformed other candidate algorithms with an accuracy of 0.92 and AUC of 0.94 in the testing dataset. In the provider comparison dataset, for "brain compression," the random forest algorithm demonstrated better accuracy (0.76 vs 0.70) and sensitivity (0.73 vs 0.43) than provider documentation. For "brain edema," the algorithm again demonstrated better accuracy (0.92 vs 0.84) and AUC (0.45 vs 0.09) than provider documentation.
Discussion: A natural language processing-based machine learning algorithm can reliably and reproducibly identify selected common neurosurgical comorbidities from radiology reports.
Conclusion: This result may justify the use of machine learning-based decision support to augment provider documentation.
Copyright: © 2024 Sastry et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Aiello FA, Judelson DR, Durgin JM, Doucet DR, Simons JP, Durocher DM, et al. A physician-led initiative to improve clinical documentation results in improved health care documentation, case mix index, and increased contribution margin. J Vasc Surg. 2018;68: 1524–1532. doi: 10.1016/j.jvs.2018.02.038 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
