

Implementation of an integrated primary care prevention and management program for chronic low back pain (LBP): patient-reported outcomes and predictors of pain interference after six months
- PMID: 38725037
- PMCID: PMC11083802
- DOI: 10.1186/s12913-024-11031-x
Implementation of an integrated primary care prevention and management program for chronic low back pain (LBP): patient-reported outcomes and predictors of pain interference after six months
Abstract
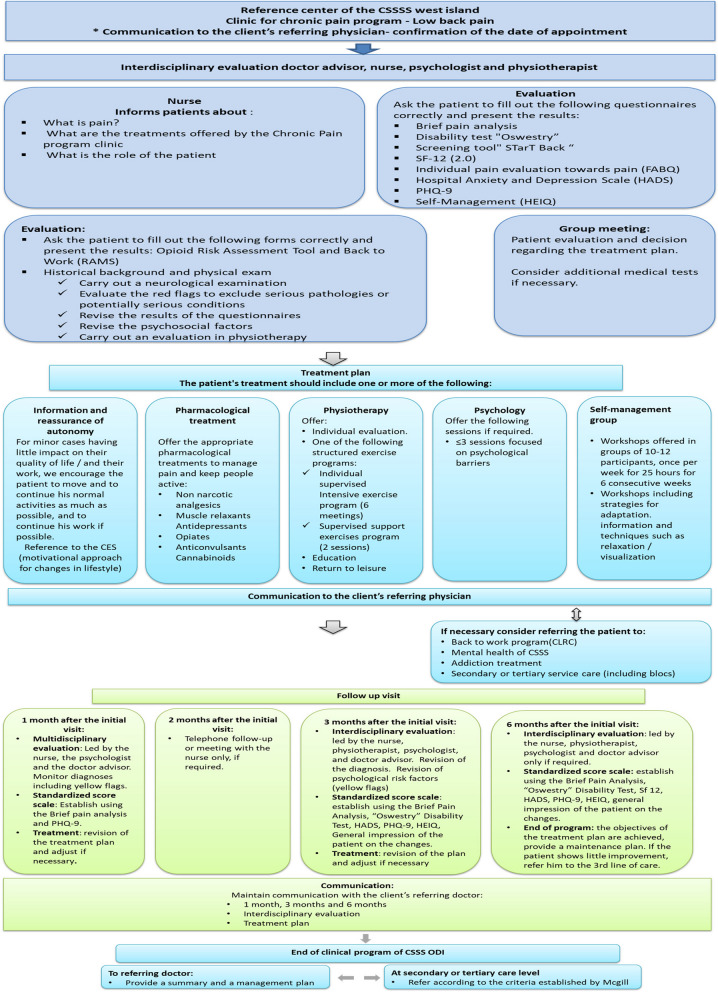
Background: Integrated primary care programs for patients living with chronic pain which are accessible, interdisciplinary, and patient-centered are needed for preventing chronicity and improving outcomes. Evaluation of the implementation and impact of such programs supports further development of primary care chronic pain management. This study examined patient-reported outcomes among individuals with low back pain (LBP) receiving care in a novel interdisciplinary primary care program.
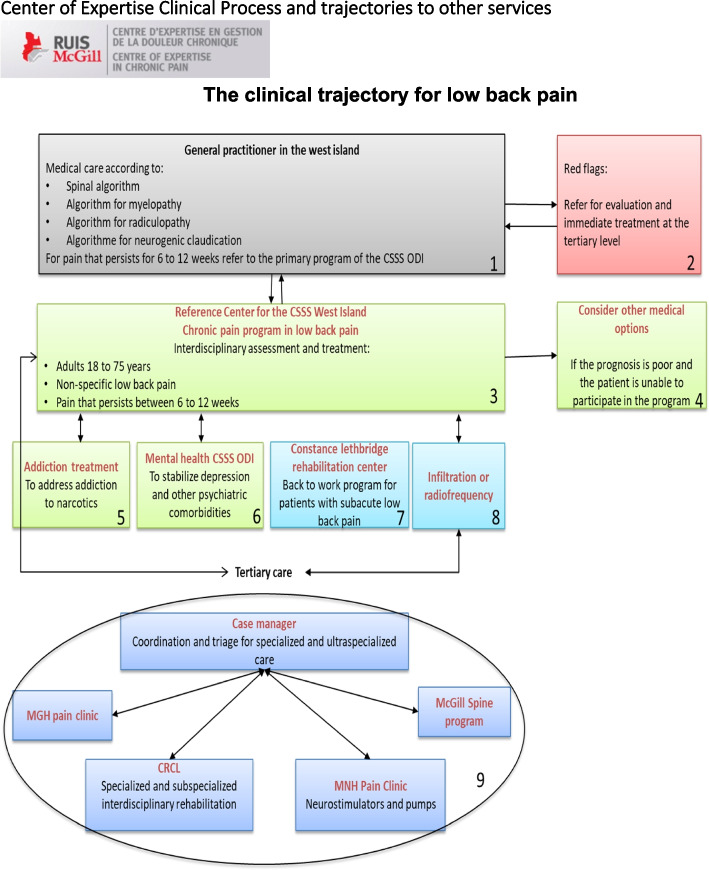
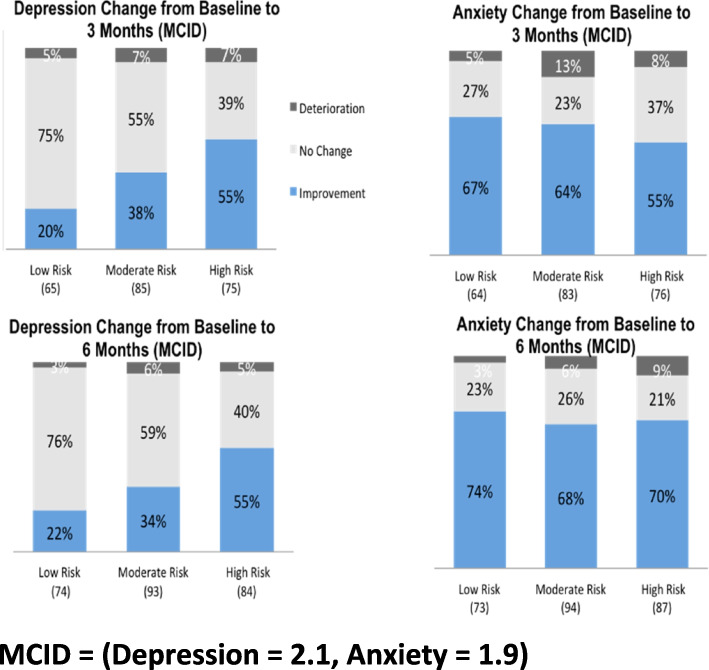
Methods: Patients were referred by primary care physicians in four regions of Quebec, Canada, and eligible patients received an evidence-based interdisciplinary pain management program over a six-month period. Patients were screened for risk of chronicity. Patient-reported outcome measures of pain interference and intensity, physical function, depression, and anxiety were evaluated at regular intervals over the six-month follow-up. A multilevel regression analysis was performed to evaluate the association between patient characteristics at baseline, including risk of chronicity, and change in pain outcomes.
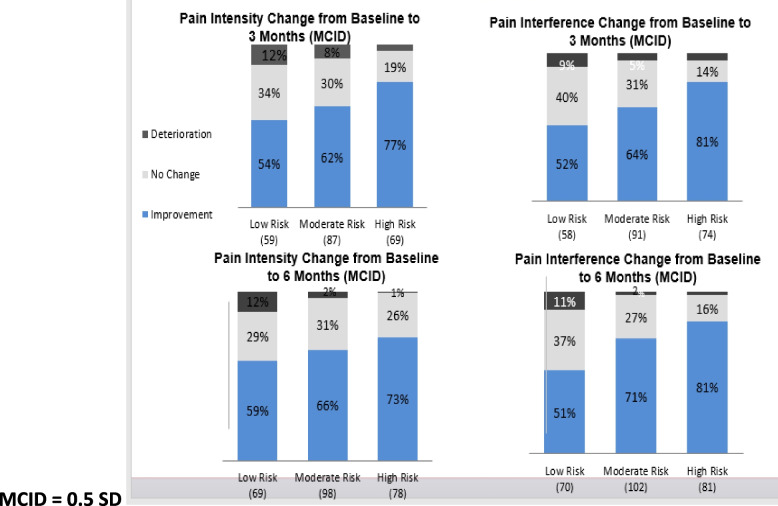
Results: Four hundred and sixty-four individuals (mean age 55.4y, 63% female) completed the program. The majority (≥ 60%) experienced a clinically meaningful improvement in pain intensity and interference at six months. Patients with moderate (71%) or high risk (81%) of chronicity showed greater improvement in pain interference than those with low risk (51%). Significant predictors of improvement in pain interference included a higher risk of chronicity, younger age, female sex, and lower baseline disability.
Conclusion: The outcomes of this novel LBP program will inform wider implementation considerations by identifying key components for further effectiveness, sustainability, and scale-up of the program.
Keywords: Chronic pain; Integrated care; Low back pain; Person-centred care; Primary care; Sub-acute pain.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Agence d'évaluation des technologies et des modes d'intervention en santé. Management of Chronic (Non-Cancer) Pain: Organization of Health Services. Montréal: AETMIS; . 2006.
-
- Reliving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research [press release]. Washington, DC: : The National Academies Press; 2011. - PubMed
-
- pain WHOstgetrc. 2004 [updated 2011/10/09/. [Available from: Available from: http://www.who.int/mediacentre/news/releases/2004/pr70/en/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
