

Which radial head fractures are best treated surgically?
- PMID: 38726982
- PMCID: PMC11099579
- DOI: 10.1530/EOR-24-0035
Which radial head fractures are best treated surgically?
Abstract
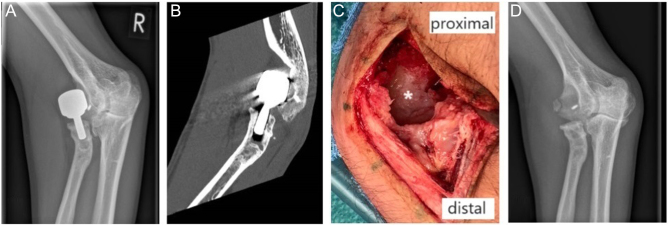
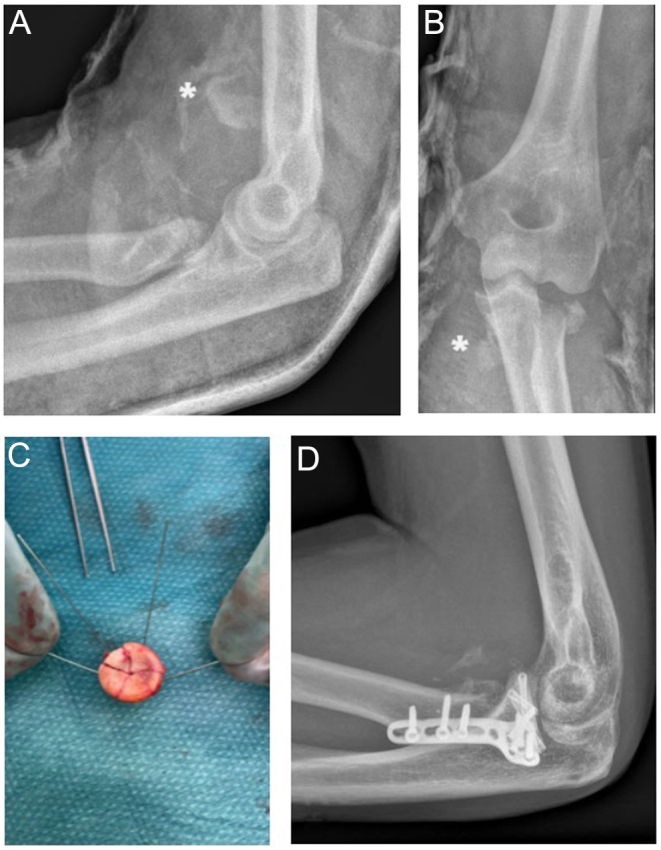
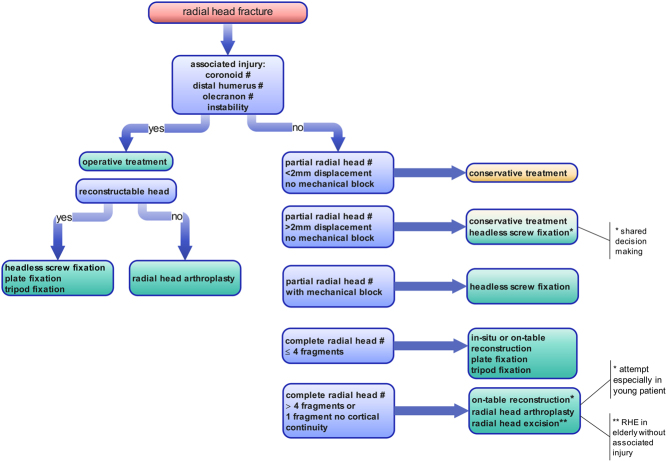
Despite the common occurrence of radial head fractures, there is still a lack of consensus on which radial head fractures should be treated surgically. The radial head is an important secondary stabilizer in almost all directions. An insufficient radial head can lead to increased instability in varus-valgus and posterolateral rotatory directions, especially in a ligament-deficient elbow. The decision to perform surgery is often not dictated by the fracture pattern alone but also by the presence of associated injury. Comminution of the radial head and complete loss of cortical contact of at least one fracture fragment are associated with a high occurrence of associated injuries. Nondisplaced and minimally displaced radial head fractures can be treated non-operatively with early mobilization. Displacement (>2 mm) of fragments in radial head fractures without a mechanical block to pronation/supination is not a clear indication for surgery. Mechanical block to pronation/supination and comminution of the fracture are indications for surgery. The following paper reviews the current literature and provides state-of-the-art guidance on which radial head fractures should be treated surgically.
Keywords: arthroplasty; open reduction internal fixation; radial head excision; radial head fractures.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of this instructional lecture
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
