

Retrogasserian trigeminal radiofrequency-thermorhizotmoy for trigeminal neuralgia
- PMID: 38727725
- PMCID: PMC11087336
- DOI: 10.1007/s00701-024-06074-2
Retrogasserian trigeminal radiofrequency-thermorhizotmoy for trigeminal neuralgia
Abstract
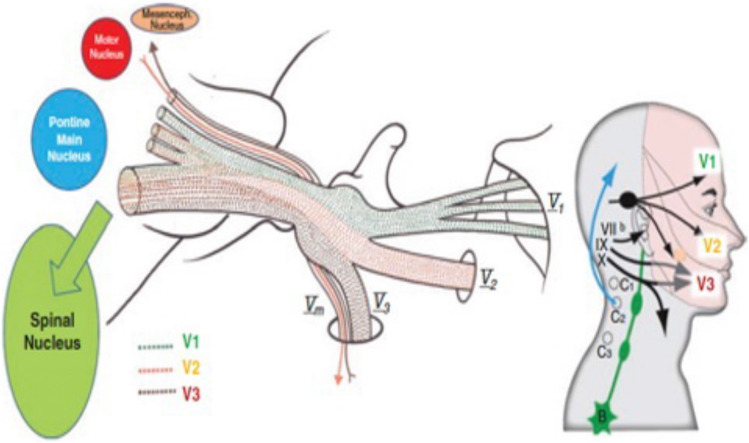
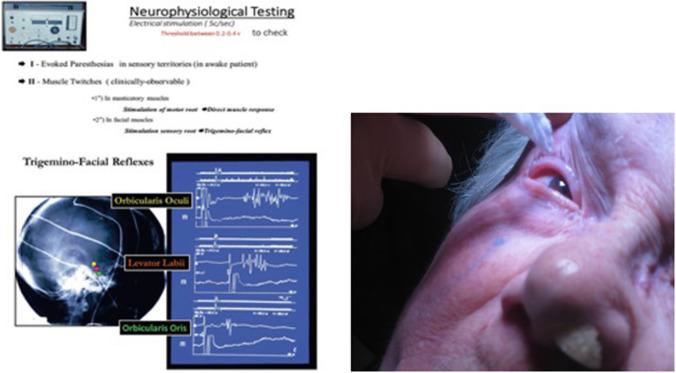
Based on a personal experience of 4200 surgeries, radiofrequency thermocoagulation is useful lesional treatment for those trigeminal neuralgias (TNs) not amenable to microvascular decompression (idiopathic or secondary TNs). Introduced through the foramen ovale, behind the trigemnial ganglion in the triangular plexus, the needle is navigated by radiology and neurophysiological testing to target the retrogasserian fibers corresponding to the trigger zone. Heating to 55-75 °C can achieve hypoesthesia without anaesthesia dolorosa if properly controlled. Depth of anaesthesia varies dynamically sedation for cannulation and lesioning, and awareness during neurophysiologic navigation. Proper technique ensures long-lasting results in more than 75% of patients.
Keywords: Hartel’s approach; Percutaneous; Rf-Thermocoagulation; Trigeminal neuralgia.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest relevant to this work.
The authors declare they have no competing interests pertaining to this work.
Figures




References
-
- Alvernia JE, Sindou MP, Dang ND, Maley JH, Mertens P (2010) Percutaneous approach to the foramen ovale: an anatomical study of the extracranial trajectory with the incorrect trajectories to be avoided. Acta Neurochir (Wien) 152(6):1043–1053. 10.1007/s00701-010-0604-y - PubMed
-
- Bernard F, Mercier P, Sindou M (2019) Morphological and functional anatomy of the trigeminal triangular plexus as an anatomical entity: a systematic review. Surg Radiol Anat 41(6):625–637. 10.1007/s00276-019-02217-8 - PubMed
-
- Hartel F (1912) Die Leitungsanasthese und Injecktionbehandlung des Ganglioni gasseri und der Trigeminusstamme Arch Klin Chir 100:627–638
-
- Kirschner M (1933) Die Punktionstechnik und die Elektrokoagulation des Ganglion Gasseri. Arch Klin Chir. 176:581–620
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
