

Revealing prognostic insights of programmed cell death (PCD)-associated genes in advanced non-small cell lung cancer
- PMID: 38728242
- PMCID: PMC11131998
- DOI: 10.18632/aging.205807
Revealing prognostic insights of programmed cell death (PCD)-associated genes in advanced non-small cell lung cancer
Abstract
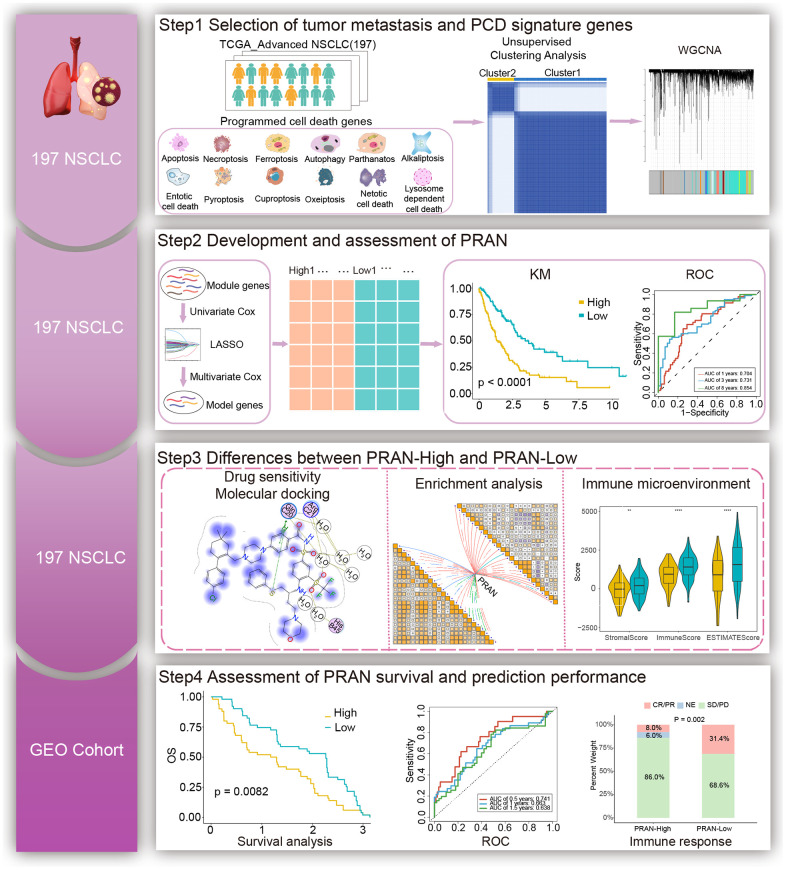
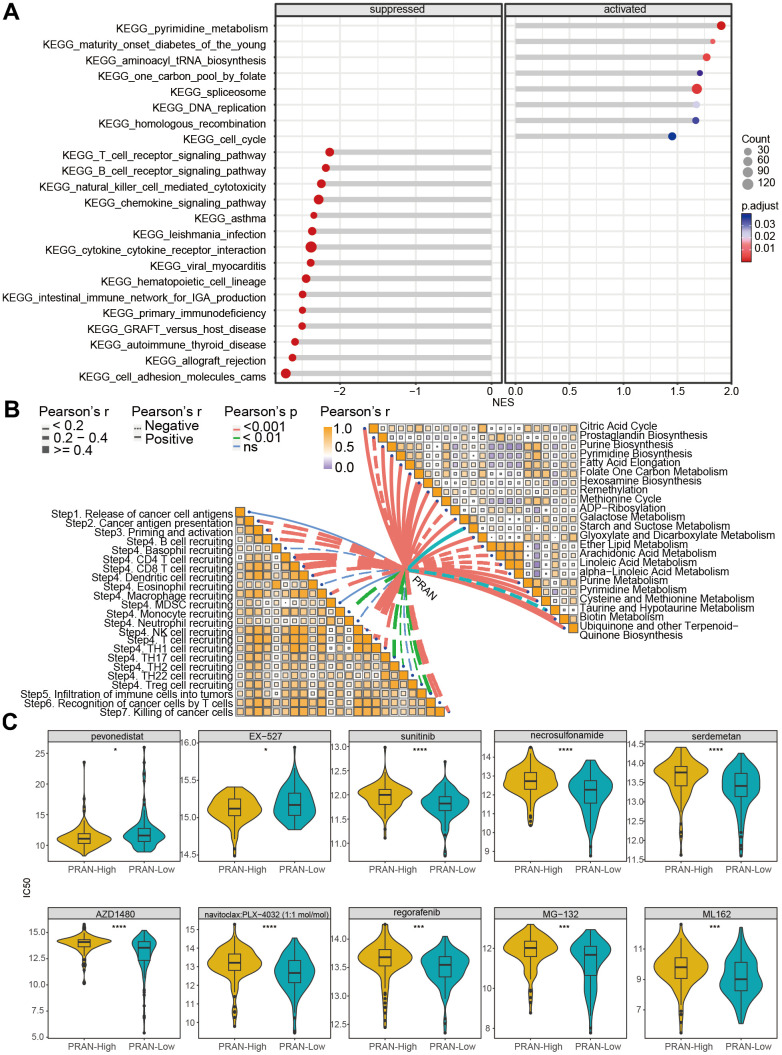
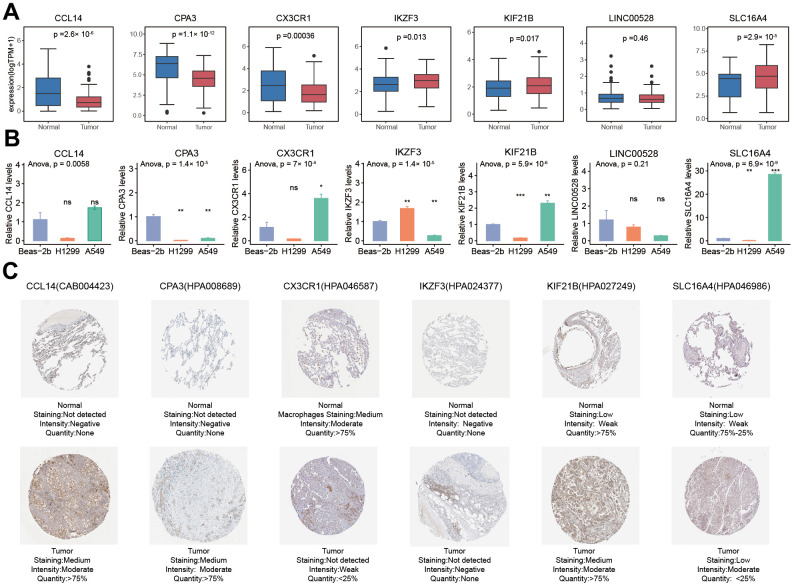
The management of patients with advanced non-small cell lung cancer (NSCLC) presents significant challenges due to cancer cells' intricate and heterogeneous nature. Programmed cell death (PCD) pathways are crucial in diverse biological processes. Nevertheless, the prognostic significance of cell death in NSCLC remains incompletely understood. Our study aims to investigate the prognostic importance of PCD genes and their ability to precisely stratify and evaluate the survival outcomes of patients with advanced NSCLC. We employed Weighted Gene Co-expression Network Analysis (WGCNA), Least Absolute Shrinkage and Selection Operator (LASSO), univariate and multivariate Cox regression analyses for prognostic gene screening. Ultimately, we identified seven PCD-related genes to establish the PCD-related risk score for the advanced NSCLC model (PRAN), effectively stratifying overall survival (OS) in patients with advanced NSCLC. Multivariate Cox regression analysis revealed that the PRAN was the independent prognostic factor than clinical baseline factors. It was positively related to specific metabolic pathways, including hexosamine biosynthesis pathways, which play crucial roles in reprogramming cancer cell metabolism. Furthermore, drug prediction for different PRAN risk groups identified several sensitive drugs explicitly targeting the cell death pathway. Molecular docking analysis suggested the potential therapeutic efficacy of navitoclax in NSCLC, as it demonstrated strong binding with the amino acid residues of C-C motif chemokine ligand 14 (CCL14), carboxypeptidase A3 (CPA3), and C-X3-C motif chemokine receptor 1 (CX3CR1) proteins. The PRAN provides a robust personalized treatment and survival assessment tool in advanced NSCLC patients. Furthermore, identifying sensitive drugs for distinct PRAN risk groups holds promise for advancing targeted therapies in NSCLC.
Keywords: PRAN risk model; RT-qPCR; advanced NSCLC; molecular docking; programmed cell death-related genes.
Conflict of interest statement
Figures








References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
