

Mitral annular disjunction and its progression during childhood in Marfan syndrome
- PMID: 38728377
- PMCID: PMC11346360
- DOI: 10.1093/ehjci/jeae125
Mitral annular disjunction and its progression during childhood in Marfan syndrome
Abstract
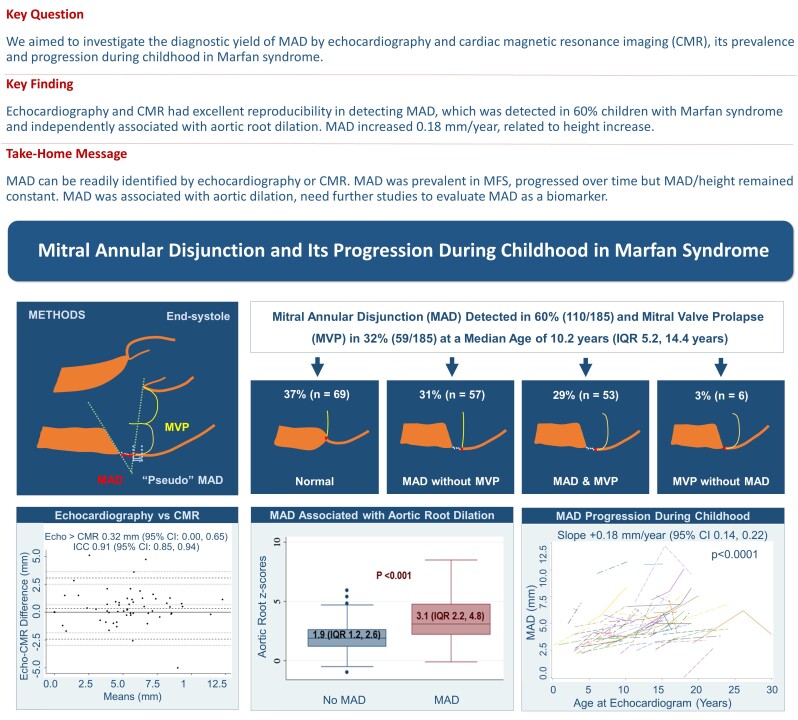
Aims: Data on mitral annular disjunction (MAD) in children with Marfan syndrome (MFS) are sparse. To investigate the diagnostic yield of MAD by echocardiography and cardiac magnetic resonance imaging (CMR), its prevalence and progression during childhood.
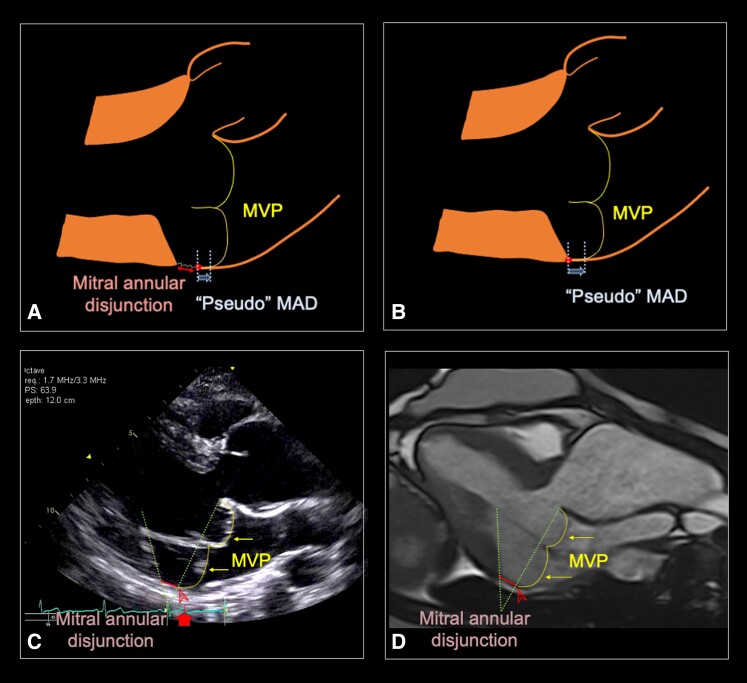
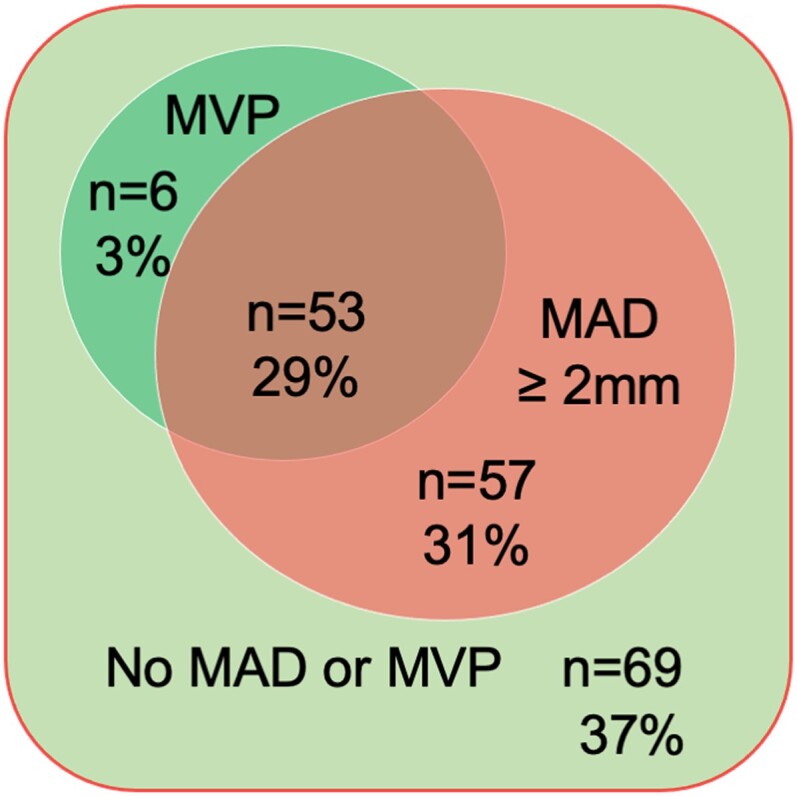
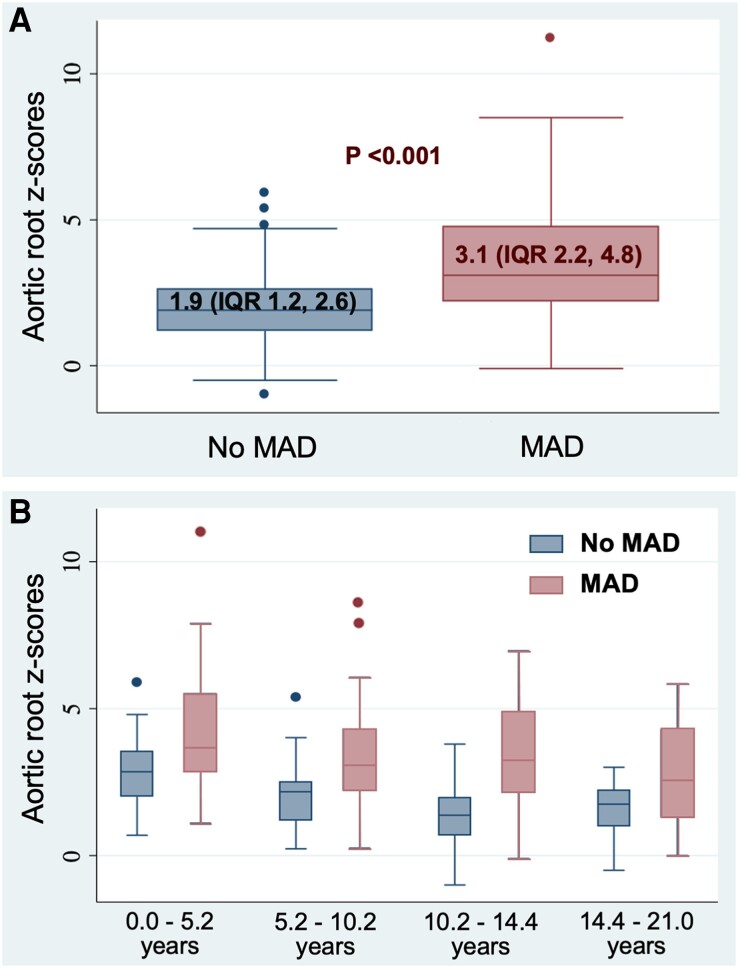
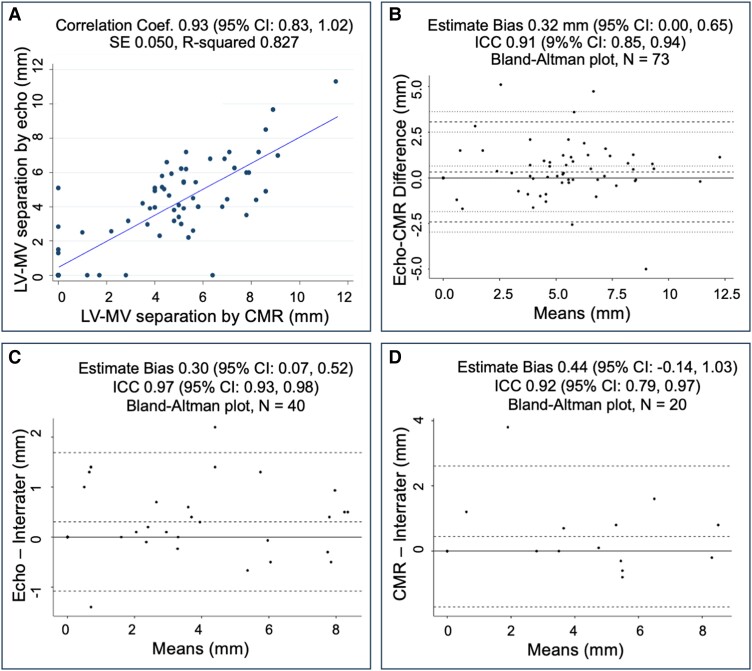
Methods and results: We included patients <21 years old with MFS, defined by 2010 Ghent criteria and a pathogenic FBN1 variant or ectopia lentis. Two readers measured systolic separation between the mitral valve (MV) posterior hinge point and left ventricular (LV) myocardium on initial and subsequent imaging. MAD was defined as MV-LV separation ≥2 mm, MV prolapse (MVP) as atrial displacement ≥2 mm. Kappa coefficients evaluated echocardiogram-CMR agreement. Bland-Altman and intraclass correlation coefficients (ICCs) assessed inter-rater and inter-modality reliability. Univariable mixed-effects linear regression was used to evaluate longitudinal changes of MAD. MAD was detected in 60% (110/185) eligible patients. MVP was present in 48% (53/110) of MAD and MAD in 90% (53/59) of MVP. MAD detection by CMR and echocardiography had 96% overall agreement (Kappa = 0.89, P < 0.001) and a 0.32 mm estimate bias (95% CI 0.00, 0.65). ICC by echocardiography, CMR, and between modalities were 0.97 (95% CI 0.93, 0.98), 0.92 (95% CI 0.79, 0.97), and 0.91 (95% CI 0.85, 0.94), respectively. MAD was associated with aortic root dilation (P < 0.001). MAD was found in children of all ages, increased +0.18 mm/year (95% CI +0.14, +0.22) during a median duration of 5.5 years (IQR 3.1, 7.5 years). MAD indexed by height yielded a constant value +0.0002 mm/m/year (95% CI -0.0002, +0.0005 mm/m/year).
Conclusion: MAD was common in pediatric MFS and was associated with aortic root dilation. MAD detection by echocardiography and CMR was highly reliable, suggesting that routine assessment in MFS is feasible. MAD was present in neonates and progressed over time but remained constant when indexing by height. Further studies are needed to evaluate MAD as a biomarker for clinical outcomes in pediatric MFS.
Keywords: Marfan syndrome; aortic root dilation; cardiac magnetic resonance imaging; children; echocardiography; mitral annular disjunction.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Bharati S, Granston AS, Liebson PR, Loeb HS, Rosen KM, Lev M. The conduction system in mitral valve prolapse syndrome with sudden death. Am Heart J 1981;101:667–70. - PubMed
-
- Hutchins GM, Moore GW, Skoog DK. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N Engl J Med 1986;314:535–40. - PubMed
-
- Tani T, Konda T, Kitai T, Ota M, Furukawa Y. Mitral annular disjunction—a new disease spectrum. Cardiol Clin 2021;39:289–94. - PubMed
-
- Basso C, Perazzolo Marra M. Mitral annulus disjunction. J Am Coll Cardiol 2018;72:1610–2. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
