

Early and extended erythropoietin monotherapy after hypoxic ischaemic encephalopathy: a multicentre double-blind pilot randomised controlled trial
- PMID: 38729748
- PMCID: PMC11503063
- DOI: 10.1136/archdischild-2024-327107
Early and extended erythropoietin monotherapy after hypoxic ischaemic encephalopathy: a multicentre double-blind pilot randomised controlled trial
Abstract
Objective: To examine the feasibility of early and extended erythropoietin monotherapy after hypoxic ischaemic encephalopathy (HIE).
Design: Double-blind pilot randomised controlled trial.
Setting: Eight neonatal units in South Asia.
Patients: Neonates (≥36 weeks) with moderate or severe HIE admitted between 31 December 2022 and 3 May 2023.
Interventions: Erythropoietin (500 U/kg daily) or to the placebo (sham injections using a screen) within 6 hours of birth and continued for 9 days. MRI at 2 weeks of age.
Main outcomes and measures: Feasibility of randomisation, drug administration and assessment of brain injury using MRI.
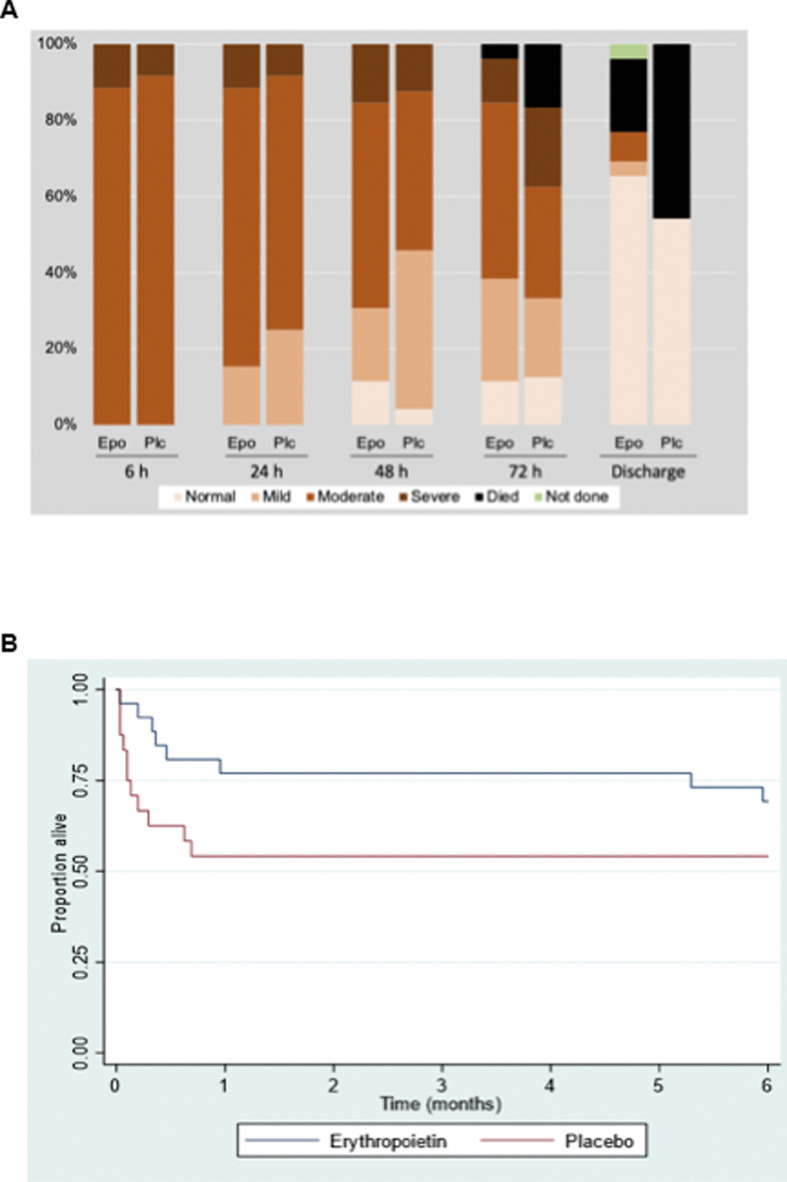
Results: Of the 154 neonates screened, 56 were eligible; 6 declined consent and 50 were recruited; 43 (86%) were inborn. Mean (SD) age at first dose was 4.4 (1.2) hours in erythropoietin and 4.1 (1.0) hours in placebo. Overall mortality at hospital discharge occurred in 5 (19%) vs 11 (46%) (p=0.06), and 3 (13%) vs 9 (40.9%) (p=0.04) among those with moderate encephalopathy in the erythropoietin and placebo groups. Moderate or severe injury to basal ganglia, white matter and cortex occurred in 5 (25%) vs 5 (38.5%); 14 (70%) vs 11 (85%); and 6 (30%) vs 2 (15.4%) in the erythropoietin and placebo group, respectively. Sinus venous thrombosis was seen in two (10%) neonates in the erythropoietin group and none in the control group.
Conclusions: Brain injury and mortality after moderate or severe HIE are high in South Asia. Evaluation of erythropoietin monotherapy using MRI to examine treatment effects is feasible in these settings.
Trial registration number: NCT05395195.
Keywords: Global Health; Intensive Care Units, Neonatal; Magnetic Resonance Imaging; Neonatology; Neurology.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical