

Effect of immediate initiation of invasive ventilation on mortality in acute hypoxemic respiratory failure: a target trial emulation
- PMID: 38730306
- PMCID: PMC11088053
- DOI: 10.1186/s13054-024-04926-y
Effect of immediate initiation of invasive ventilation on mortality in acute hypoxemic respiratory failure: a target trial emulation
Abstract
Purpose: Invasive ventilation is a fundamental treatment in intensive care but its precise timing is difficult to determine. This study aims at assessing the effect of initiating invasive ventilation versus waiting, in patients with hypoxemic respiratory failure without immediate reason for intubation on one-year mortality.
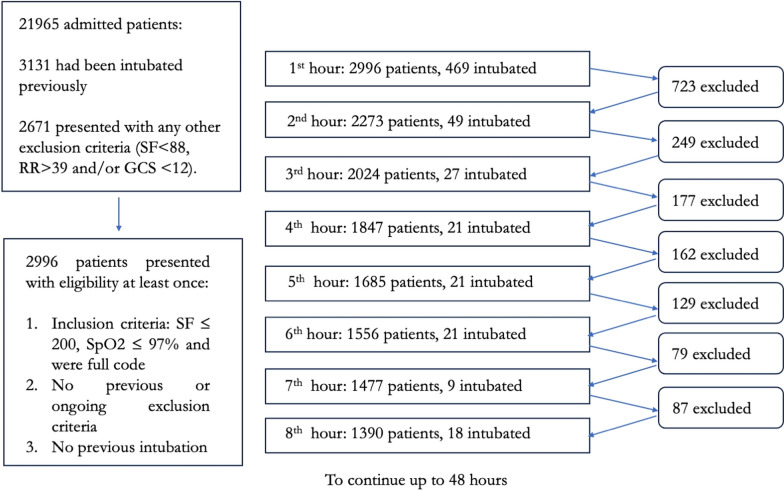
Methods: Emulation of a target trial to estimate the benefit of immediately initiating invasive ventilation in hypoxemic respiratory failure, versus waiting, among patients within the first 48-h of hypoxemia. The eligible population included non-intubated patients with SpO2/FiO2 ≤ 200 and SpO2 ≤ 97%. The target trial was emulated using a single-center database (MIMIC-IV) which contains granular information about clinical status. The hourly probability to receive mechanical ventilation was continuously estimated. The hazard ratios for the primary outcome, one-year mortality, and the secondary outcome, 30-day mortality, were estimated using weighted Cox models with stabilized inverse probability weights used to adjust for measured confounding.
Results: 2996 Patients fulfilled the inclusion criteria of whom 792 were intubated within 48 h. Among the non-invasive support devices, the use of oxygen through facemask was the most common (75%). Compared to patients with the same probability of intubation but who were not intubated, intubation decreased the hazard of dying for the first year after ICU admission HR 0.81 (95% CI 0.68-0.96, p = 0.018). Intubation was associated with a 30-day mortality HR of 0.80 (95% CI 0.64-0.99, p = 0.046).
Conclusion: The initiation of mechanical ventilation in patients with acute hypoxemic respiratory failure reduced the hazard of dying in this emulation of a target trial.
Keywords: Artificial respiration; Critical care; Respiratory insufficiency.
© 2024. The Author(s).
Conflict of interest statement
RMA discloses speaker fees from Medtronic and Fisher & Paykel; all outside the submitted work. LB’s laboratory received grants from Medtronic, Draeger, Stimit, Vitalaire and equipment from Fisher Paykel, Philips and Sentec. All the other authors disclose no conflicts of interest.
Figures


Comment in
-
Effect of initiation of invasive ventilation in acute hypoxemic respiratory failure using sequential trials: treatment efficacy instead of timing.Crit Care. 2025 Jun 3;29(1):221. doi: 10.1186/s13054-025-05464-x. Crit Care. 2025. PMID: 40462175 Free PMC article. No abstract available.
References
-
- Frat J-P, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185–96. 10.1056/NEJMoa1503326. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
