

Minimal residual disease profiling predicts pathological complete response in esophageal squamous cell carcinoma
- PMID: 38730415
- PMCID: PMC11084057
- DOI: 10.1186/s12943-024-02006-x
Minimal residual disease profiling predicts pathological complete response in esophageal squamous cell carcinoma
Abstract
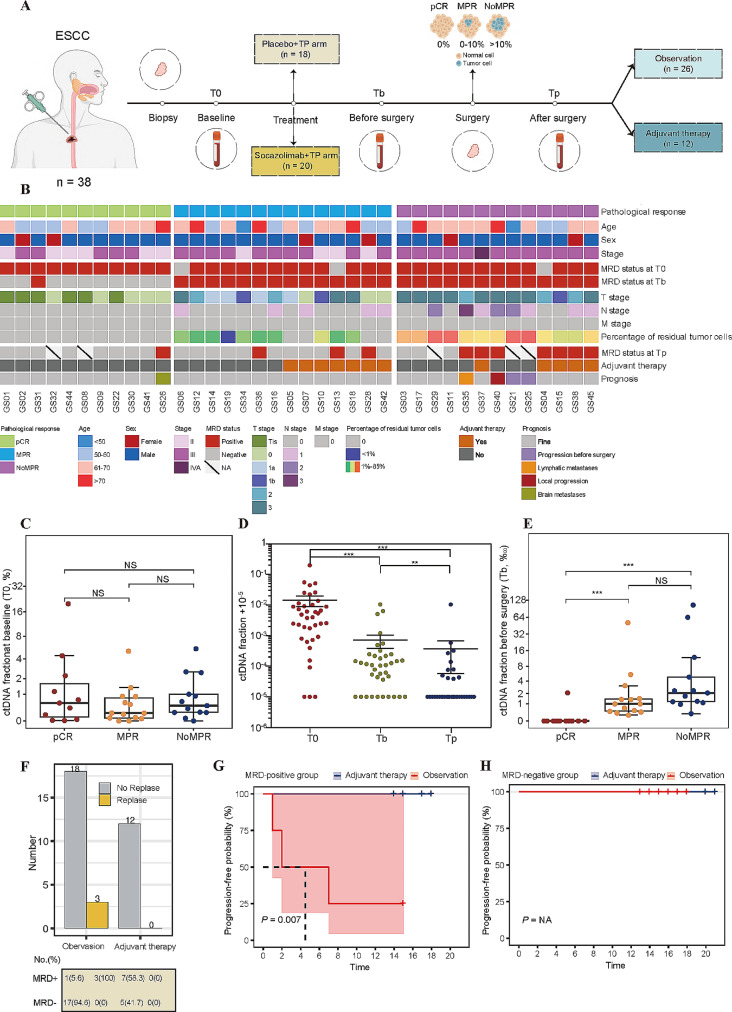
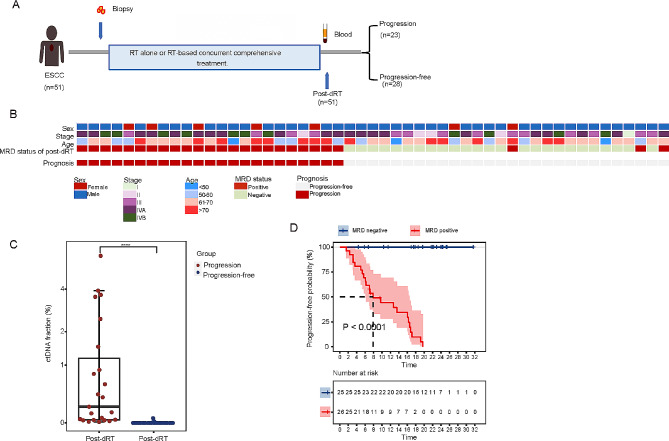
Accurate presurgical prediction of pathological complete response (pCR) can guide treatment decisions, potentially avoiding unnecessary surgeries and improving the quality of life for cancer patients. We developed a minimal residual disease (MRD) profiling approach with enhanced sensitivity and specificity for detecting minimal tumor DNA from cell-free DNA (cfDNA). The approach was validated in two independent esophageal squamous cell carcinoma (ESCC) cohorts. In a cohort undergoing neoadjuvant, surgical, and adjuvant therapy (NAT cohort), presurgical MRD status precisely predicted pCR. All MRD-negative cases (10/10) were confirmed as pCR by pathological evaluation on the resected tissues. In contrast, MRD-positive cases included all the 27 non-pCR cases and only one pCR case (10/10 vs 1/28, P < 0.0001, Fisher's exact test). In a definitive radiotherapy cohort (dRT cohort), post-dRT MRD status was closely correlated with patient prognosis. All MRD-negative patients (25/25) remained progression-free during the follow-up period, while 23 of the 26 MRD-positive patients experienced disease progression (25/25 vs 3/26, P < 0.0001, Fisher's exact test; progression-free survival, P < 0.0001, log-rank test). The MRD profiling approach effectively predicted the ESCC patients who would achieve pCR with surgery and those likely to remain progression-free without surgery. This suggests that the cancer cells in these MRD-negative patients have been effectively eliminated and they could be suitable candidates for a watch-and-wait strategy, potentially avoiding unnecessary surgery.
Keywords: Adjuvant therapy; Definitive radiotherapy; Esophageal squamous cell carcinoma; Minimal residual disease; Neoadjuvant therapy; Pathological complete response.
© 2024. The Author(s).
Conflict of interest statement
Y.J. is one of the cofounders of Genetron Holdings, has owner interest in Genetron Holdings, and receives royalties from Genetron. Other authors declare no conflict of interest.
Figures
References
-
- Samson P, Robinson C, Bradley J, Lockhart AC, Puri V, Broderick S, et al. Neoadjuvant chemotherapy versus Chemoradiation Prior to Esophagectomy: impact on rate of complete pathologic response and survival in Esophageal Cancer patients. J Thorac Oncol. 2016;11(12):2227–37. doi: 10.1016/j.jtho.2016.07.031. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 2021YFC2500900/National Key R&D Program of China
- 82225033/National Natural Science Foundation Fund
- 2021-I2M-1-015, 2021-1-I2M-018, and 2021-I2M-1-067/Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS)
- 2021-I2M-1-015, 2021-1-I2M-018, and 2021-I2M-1-067/Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS)
- 2022-RC310-08/Non-profit central research institute fund of Chinese Academy of Medical Sciences
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
