

The Evolving Classification of Meningiomas: Integration of Molecular Discoveries to Inform Patient Care
- PMID: 38730704
- PMCID: PMC11083836
- DOI: 10.3390/cancers16091753
The Evolving Classification of Meningiomas: Integration of Molecular Discoveries to Inform Patient Care
Abstract
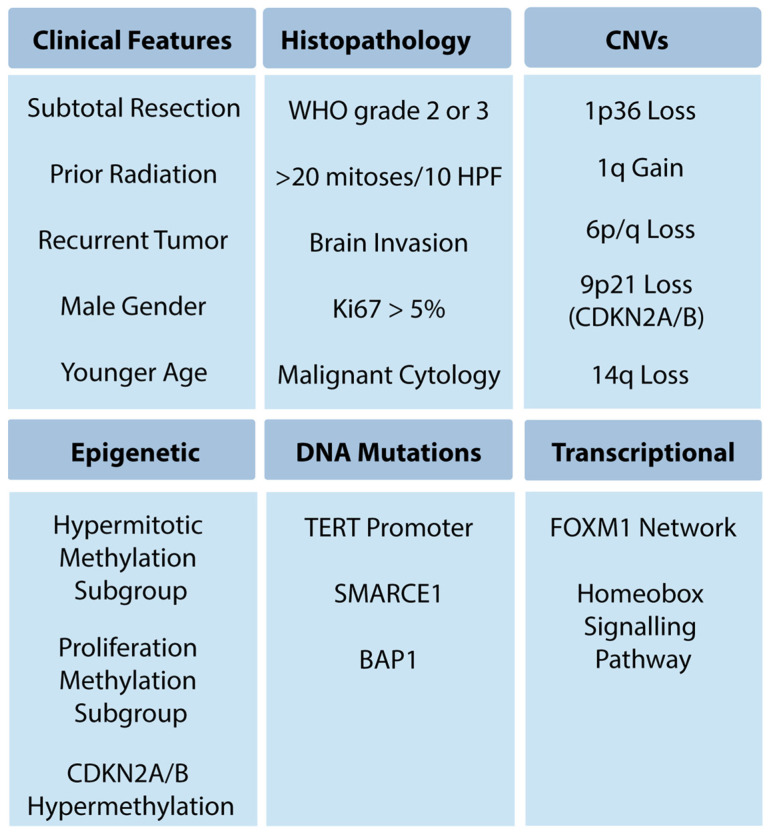
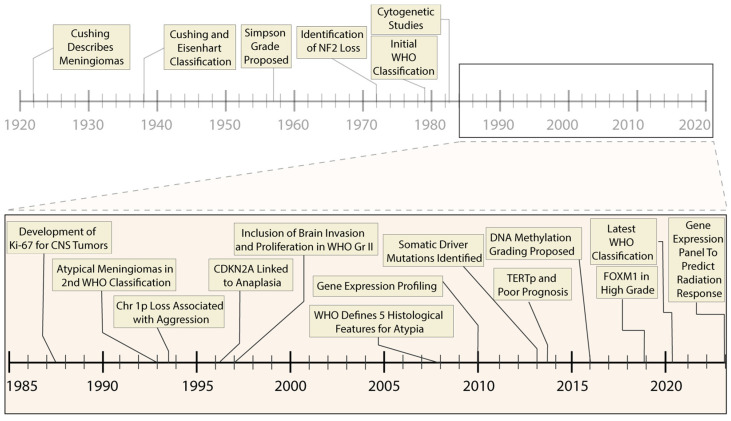
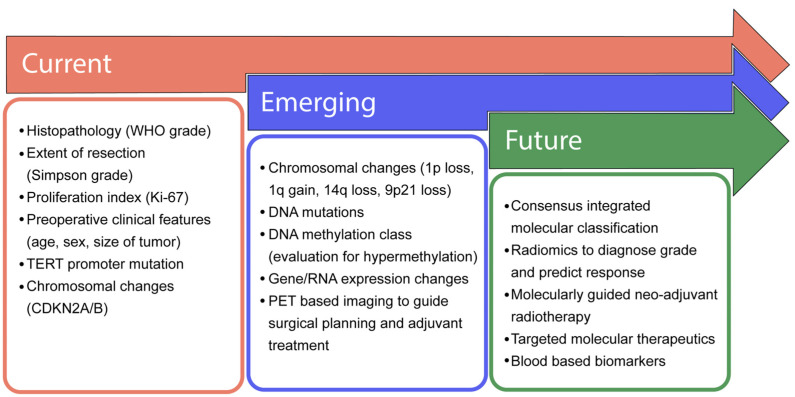
Meningioma classification and treatment have evolved over the past eight decades. Since Bailey, Cushing, and Eisenhart's description of meningiomas in the 1920s and 1930s, there have been continual advances in clinical stratification by histopathology, radiography and, most recently, molecular profiling, to improve prognostication and predict response to therapy. Precise and accurate classification is essential to optimizing management for patients with meningioma, which involves surveillance imaging, surgery, primary or adjuvant radiotherapy, and consideration for clinical trials. Currently, the World Health Organization (WHO) grade, extent of resection (EOR), and patient characteristics are used to guide management. While these have demonstrated reliability, a substantial number of seemingly benign lesions recur, suggesting opportunities for improvement of risk stratification. Furthermore, the role of adjuvant radiotherapy for grade 1 and 2 meningioma remains controversial. Over the last decade, numerous studies investigating the molecular drivers of clinical aggressiveness have been reported, with the identification of molecular markers that carry clinical implications as well as biomarkers of radiotherapy response. Here, we review the historical context of current practices, highlight recent molecular discoveries, and discuss the challenges of translating these findings into clinical practice.
Keywords: WHO grade; copy number variant; gene expression panel; history; meningioma; methylation; molecular.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ostrom Q.T., Price M., Neff C., Cioffi G., Waite K.A., Kruchko C., Barnholtz-Sloan J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2016–2020. Neuro-Oncology. 2023;25((Suppl. S4)):iv1–iv99. doi: 10.1093/neuonc/noad149. - DOI - PMC - PubMed
-
- Cushing H., Eisenhardt L. Meningiomas, Their Classification, Regional Behaviour, Life History, and Surgical End Results. Charles C Thomas; Springfield, IL, USA: 1938.
-
- Cushing H. The meningiomas (dural endotheliomas): Their source, and favoured seats of origin1. Brain. 1922;45:282–316. doi: 10.1093/brain/45.2.282. - DOI
-
- Bailey P. The origin and nature of meningeal tumors. Am. J. Cancer. 1931;15:15–54.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
