

Radiological Classification and Management Algorithm of Petrous Apex Cholesterol Granuloma
- PMID: 38731034
- PMCID: PMC11084343
- DOI: 10.3390/jcm13092505
Radiological Classification and Management Algorithm of Petrous Apex Cholesterol Granuloma
Abstract
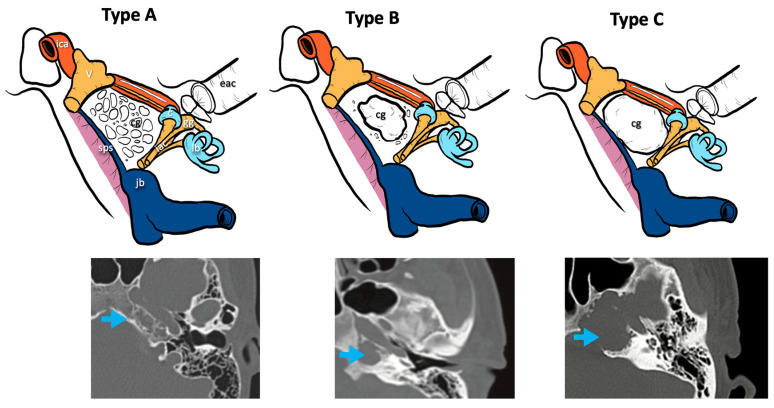
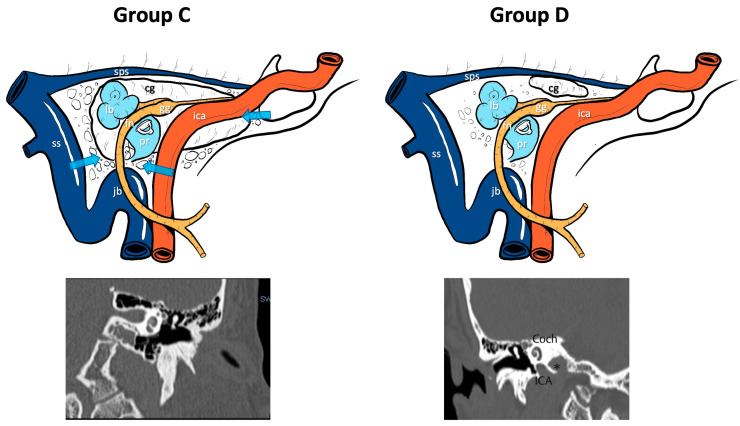
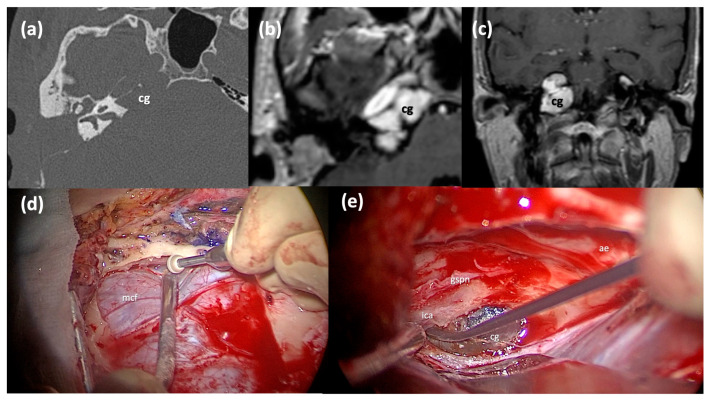
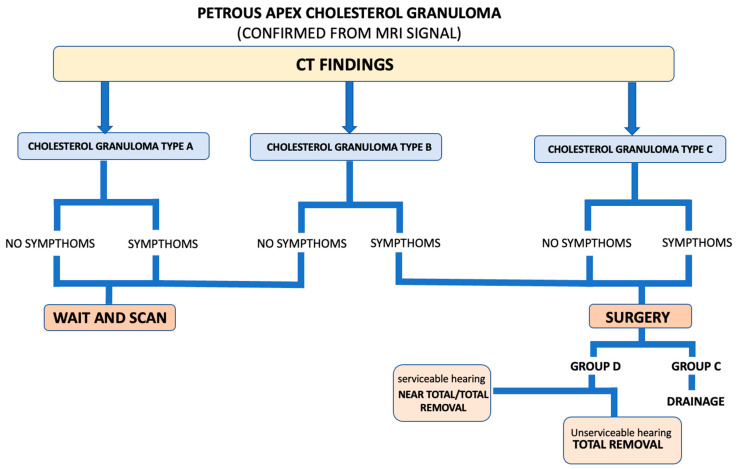
Background: Petrous apex cholesterol granulomas (PACGs) are benign inflammatory cystic lesions of the temporal bone. Usually, asymptomatic patients may develop symptoms as the lesions expand. The diagnosis is based on both CT and MRI scans and the management relies on "wait and scan" or surgery. This paper aims at evaluating surgical outcomes and proposing a CT-based classification and a management algorithm. Methods: Patients with PACGs who were surgically treated between 2014 and 2024 were included. Symptoms, imaging, approach type and complications were considered. CT scans were classified as Type A (preserved apex cellularity), Type B (erosion of the apex cellularity), and Type C (involvement of the noble structures bone boundaries). The possible connection of the lesion with the infracochlear, perilabyrinthine and sphenoidal cellularity was assessed. Results: Nineteen patients with symptoms like diplopia, headache and sensorineural hearing loss were included. According to our classification, 1/19 patients was Type A, 4/19 were Type B and 14/19 were Type C. Five patients underwent a total resection, seven a subtotal and seven a surgical drainage. Only two complications were recorded, and 17/19 patients showed symptom regression and stability during follow-up. Conclusions: While the management of PACGs is still controversial, according to our classification and surgical outcomes, Type A, being mostly asymptomatic, should be managed with "wait and scan", Type B should undergo surgery when symptoms are present, while Type C should always undergo surgery because of their invasiveness and potential complications. When possible, a drainage should be attempted; otherwise, a surgical resection is chosen, and its completeness depends on the preoperative general and hearing status.
Keywords: cholesterol granuloma; computed tomography; drainage; petrous apex; surgical excision; temporal bone.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Nemade S.V., Shinde K.J., editors. Granulomatous Diseases in Otorhinolaryngology, Head and Neck. Springer; Singapore: 2021. Cholesterol Granuloma; pp. 251–257.
-
- Isaacson B., Kutz J.W., Roland P.S. Cholesterol Granuloma. In: Kountakis S.E., editor. Encyclopedia of Otolaryngology, Head and Neck Surgery. Springer; Berlin/Heidelberg, Germany: 2013. pp. 430–436.
-
- Hoeffner E., Mukherji S., Gandhi G., Gomez-Hassan D. Temporal Bone Imaging. Thieme; New York, NY, USA: 2022. pp. 244–253.
LinkOut - more resources
Full Text Sources
Miscellaneous
