

Pituitary Apoplexy: An Updated Review
- PMID: 38731037
- PMCID: PMC11084238
- DOI: 10.3390/jcm13092508
Pituitary Apoplexy: An Updated Review
Abstract
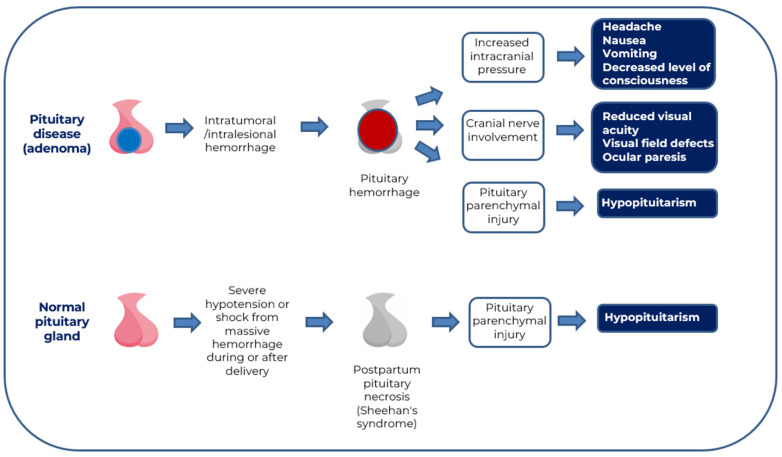
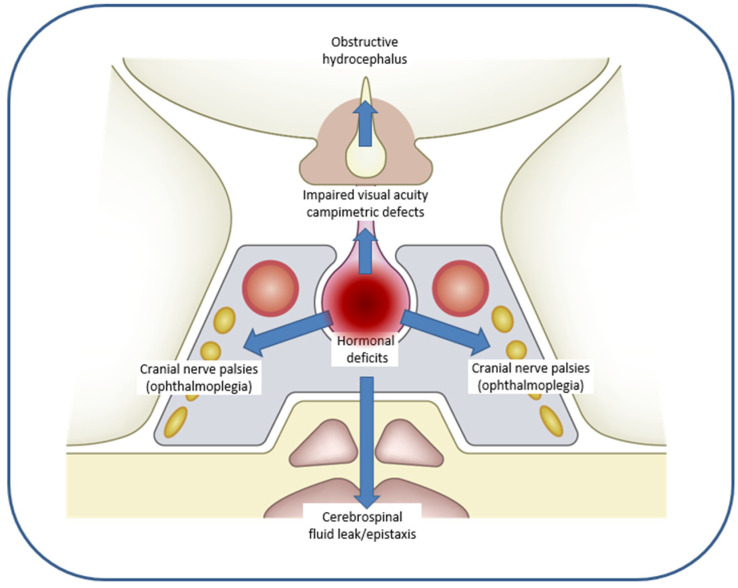
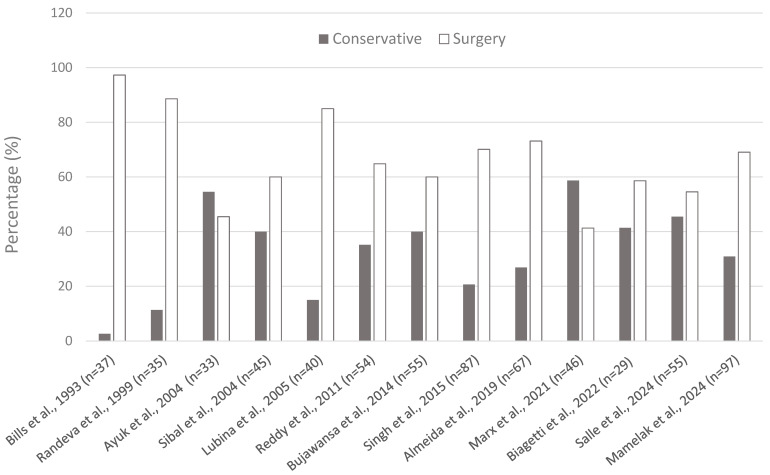
Pituitary apoplexy (PA) is an acute, life-threatening clinical syndrome caused by hemorrhage and/or infarction of the pituitary gland. It is clinically characterized by the sudden onset of headache. Depending on the severity, it may also be accompanied by nausea, vomiting, visual disturbances, varying degrees of adenohypophyseal hormone deficiency, and decreased level of consciousness. Corticotropic axis involvement may result in severe hypotension and contribute to impaired level of consciousness. Precipitating factors are present in up to 30% of cases. PA may occur at any age and sometimes develops during pregnancy or the immediate postpartum period. PA occurs more frequently in men aged 50-60, being rare in children and adolescents. It can develop in healthy pituitary glands or those affected by inflammation, infection, or tumor. The main cause of PA is usually spontaneous hemorrhage or infarction of a pituitary adenoma (pituitary neuroendocrine tumor, PitNET). It is a medical emergency requiring immediate attention and, in many cases, urgent surgical intervention and long-term follow-up. Although the majority of patients (70%) require surgery, about one-third can be treated conservatively, mainly by monitoring fluid and electrolyte levels and using intravenous glucocorticoids. There are scoring systems for PA with implications for management and therapeutic outcomes that can help guide therapeutic decisions. Management of PA requires proper evaluation and long-term follow-up by a multidisciplinary team with expertise in pituitary pathology. The aim of the review is to summarize and update the most relevant aspects of the epidemiology, etiopathogenesis, pathophysiology, clinical presentation and clinical forms, diagnosis, therapeutic strategies, and prognosis of PA.
Keywords: conservative management; hemorrhage; hypopituitarism; infarction; pituitary apoplexy; pituitary gland; surgery.
Conflict of interest statement
The author declare no conflict of interest.
Figures

Similar articles
-
Pituitary Apoplexy in Patients with Pituitary Neuroendocrine Tumors (PitNET).Biomedicines. 2023 Feb 23;11(3):680. doi: 10.3390/biomedicines11030680. Biomedicines. 2023. PMID: 36979658 Free PMC article. Review.
-
[Clinical practice guideline for the diagnosis and treatment of pituitary apoplexy].Endocrinol Nutr. 2013 Dec;60(10):582.e1-582.e12. doi: 10.1016/j.endonu.2013.04.013. Epub 2013 Sep 14. Endocrinol Nutr. 2013. PMID: 24041671 Spanish.
-
Diagnosis and management of pituitary apoplexy: a Tunisian data.Chin Neurosurg J. 2023 Jul 1;9(1):17. doi: 10.1186/s41016-023-00331-6. Chin Neurosurg J. 2023. PMID: 37391784 Free PMC article.
-
Pituitary apoplexy during pregnancy: a rare, but dangerous headache.J Endocrinol Invest. 2014 Sep;37(9):789-97. doi: 10.1007/s40618-014-0095-4. Epub 2014 Jun 11. J Endocrinol Invest. 2014. PMID: 24916564 Review.
-
Gestational pituitary apoplexy: Case series and review of the literature.J Gynecol Obstet Hum Reprod. 2019 Dec;48(10):873-881. doi: 10.1016/j.jogoh.2019.05.005. Epub 2019 May 3. J Gynecol Obstet Hum Reprod. 2019. PMID: 31059861 Review.
Cited by
-
An Update on Advances in Hypopituitarism: Etiology, Diagnosis, and Current Management.J Clin Med. 2024 Oct 16;13(20):6161. doi: 10.3390/jcm13206161. J Clin Med. 2024. PMID: 39458112 Free PMC article. Review.
-
A Complex Case of Pituitary Apoplexy Mimicking a Stroke: A Case Report With a Review of the Literature.Cureus. 2024 Jul 25;16(7):e65332. doi: 10.7759/cureus.65332. eCollection 2024 Jul. Cureus. 2024. PMID: 39184687 Free PMC article.
-
Pituitary Apoplexy in a Non-Functioning PitNET After Cabergoline Use: Case Report and Review of the Literature.J Clin Med. 2025 Jul 17;14(14):5089. doi: 10.3390/jcm14145089. J Clin Med. 2025. PMID: 40725781 Free PMC article. Review.
-
Gestational Pituitary Apoplexy With Persistent Hypogonadotropic Hypogonadism.AACE Endocrinol Diabetes. 2025 Apr 22;12(2):89-92. doi: 10.1016/j.aed.2025.04.004. eCollection 2025 Jul-Aug. AACE Endocrinol Diabetes. 2025. PMID: 40786986 Free PMC article.
-
Recurrent Aseptic Meningitis Revealing Primitive Pituitary Abscess.Cureus. 2025 Feb 5;17(2):e78537. doi: 10.7759/cureus.78537. eCollection 2025 Feb. Cureus. 2025. PMID: 40062105 Free PMC article.
References
-
- Bailey P. Pathological Report of a Case of Acromegaly, with Special Reference to the Lesions in the Hypophysis Cerebri and in the Thyroid Gland; and a Case of Haemorrhage in to the Pituitary. Phila. Med. J. 1898;1:789–792.
Publication types
LinkOut - more resources
Full Text Sources
