

Abnormal Static Sagittal Cervical Curvatures following Motor Vehicle Collisions: A Retrospective Case Series of 41 Patients before and after a Crash Exposure
- PMID: 38732372
- PMCID: PMC11082978
- DOI: 10.3390/diagnostics14090957
Abnormal Static Sagittal Cervical Curvatures following Motor Vehicle Collisions: A Retrospective Case Series of 41 Patients before and after a Crash Exposure
Abstract
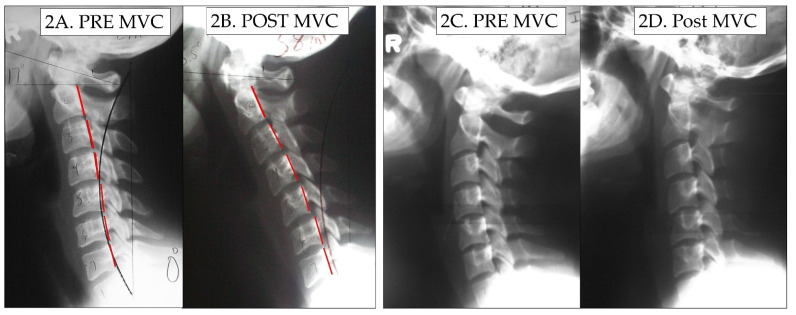
Previous investigations have found a correlation between abnormal curvatures and a variety of patient complaints such as cervical pain and disability. However, no study has shown that loss of the cervical curve is a direct result of exposure to a motor vehicle collision (MVC). This investigation presents a retrospective consecutive case series of patients with both a pre-injury cervical lateral radiograph (CLR) and a post-injury CLR after exposure to an MVC. Computer analysis of digitized vertebral body corners on CLRs was performed to investigate the possible alterations in the geometric alignment of the sagittal cervical curve.
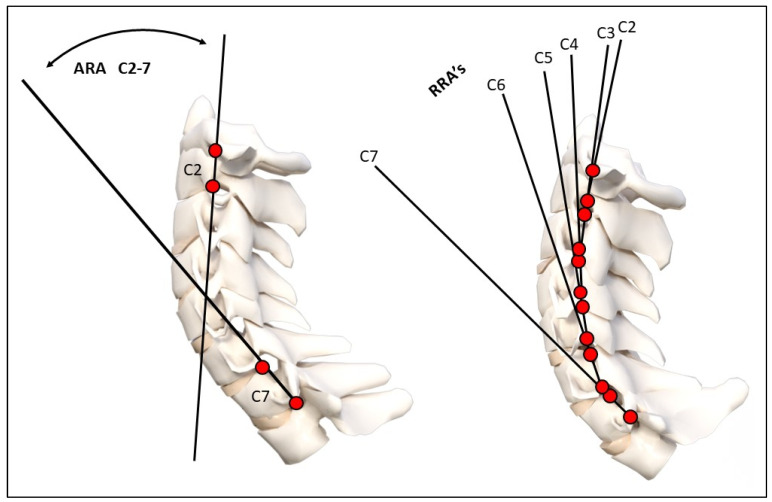
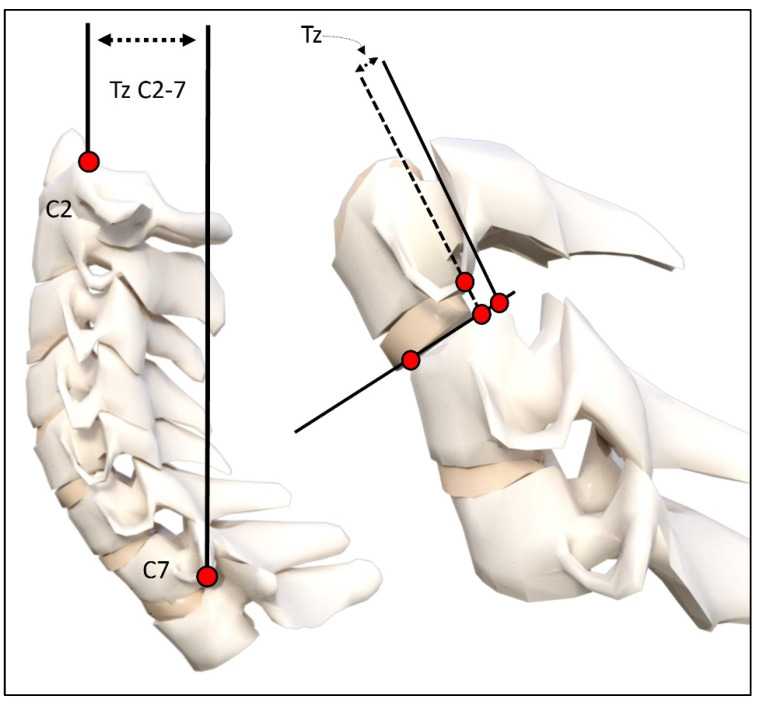
Methods: Three spine clinic records were reviewed over a 2-year period, looking for patients where both an initial lateral cervical X-ray and an examination were performed prior to the patient being exposed to a MVC; afterwards, an additional exam and radiographic analysis were obtained. A total of 41 patients met the inclusion criteria. Examination records of pain intensity on numerical pain rating scores (NPRS) and neck disability index (NDI), if available, were analyzed. The CLRs were digitized and modeled in the sagittal plane using curve fitting and the least squares error approach. Radiographic variables included total cervical curve (ARA C2-C7), Chamberlain's line to horizontal (skull flexion), horizontal translation of C2 relative to C7, segmental translations (retrolisthesis and anterolisthesis), and circular modelling radii.
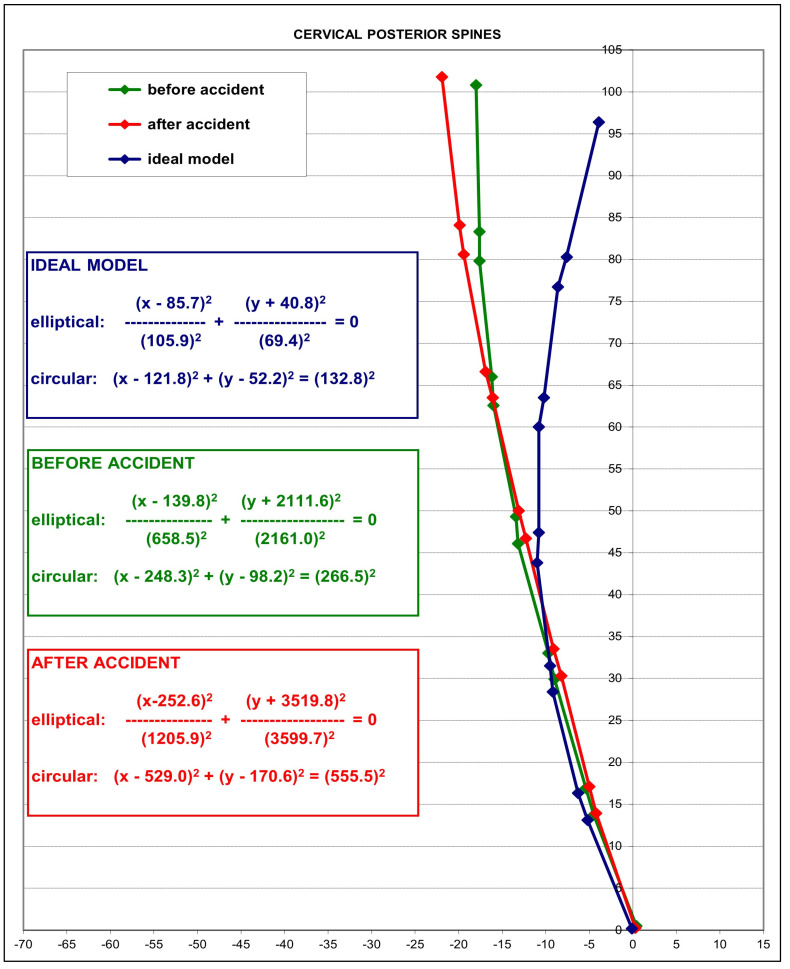
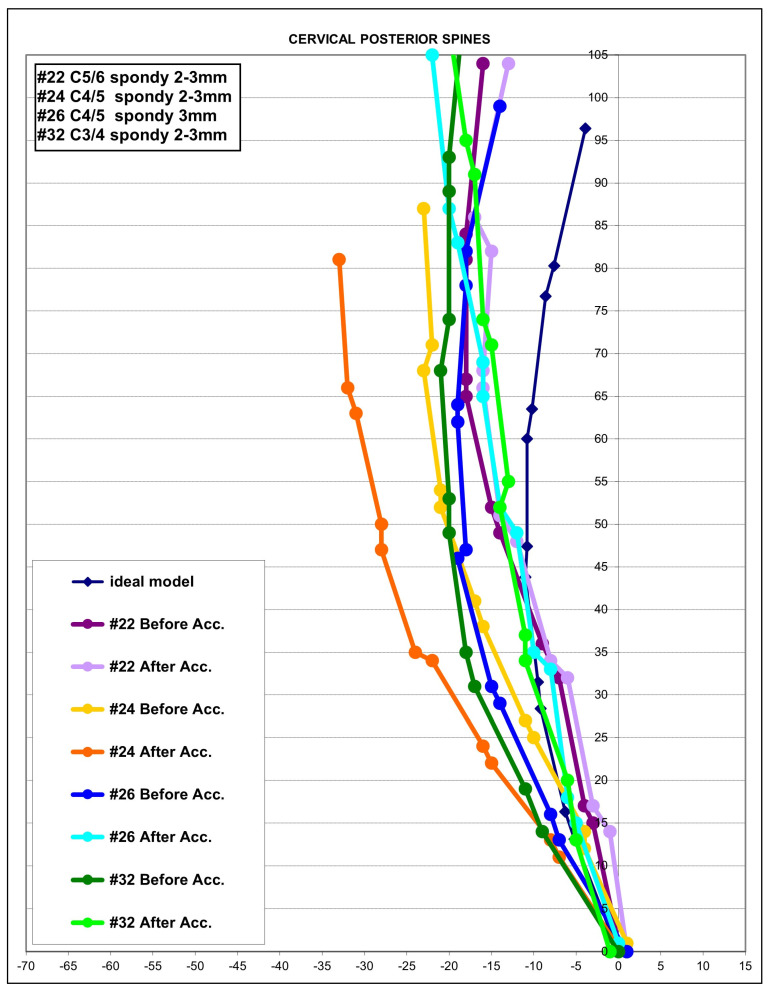
Results: There were 15 males and 26 females with an age range of 8-65 years. Most participants were drivers (28) involved in rear-end impacts (30). The pre-injury NPRS was 2.7 while the post injury was 5.0; p < 0.001. The NDI was available on 24/41 (58.5%) patients and increased after the MVC from 15.7% to 32.8%, p < 0.001. An altered cervical curvature was identified following exposure to MVC, characterized by an increase in the mean radius of curvature (265.5 vs. 555.5, p < 0.001) and an approximate 8° reduction of lordosis from C2-C7; p < 0.001. The mid-cervical spine (C3-C5) showed the greatest curve reduction with an averaged localized mild kyphosis at these levels. Four participants (10%) developed segmental translations that were just below the threshold of instability, segmental translations < 3.5 mm.
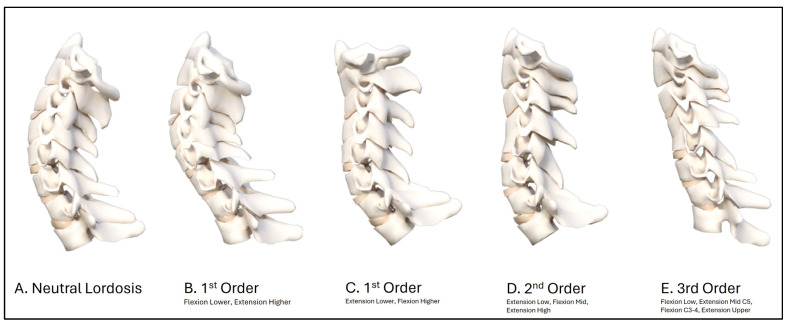
Conclusions: The post-exposure MVC cervical curvature was characterized by an increase in radius of curvature, an approximate 8° reduction in C2-C7 lordosis, a mild kyphosis of the mid-cervical spine, and a slight increase in anterior translation of C2-C7 sagittal balance. The modelling result indicates that the post-MVC cervical sagittal alignment approximates a second-order buckling alignment, indicating a significant alteration in curve geometry. Future biomechanics experiments and clinical investigations are needed to confirm these findings.
Keywords: buckling; cervical lateral radiograph; cervical lordosis; motor vehicle collision; neck pain; trauma.
Conflict of interest statement
Authors E.A.K. and I.M.M. declare no competing interests. J.W.H. is a compensated researcher for CBP Non-Profit, Inc. P.A.O. is a compensated consultant for Chiropractic BioPhysics, NonProfit, Inc. J.R.F. is the CEO of PostureCo, Inc., and receives compensation for the sale of PostureRay® software; this software was not used in this investigation. D.E.H. is the CEO of Chiropractic BioPhysics® (CBP®) and provides post-graduate education to healthcare providers and physicians. Spine rehabilitation devices are distributed through his company; none of these devices were used in this manuscript. D.E.H. is the president of CBP Non-Profit, Inc., a not-for-profit spine research foundation.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
