

The Impact of a Nutritional Intervention on Glycemic Control and Cardiovascular Risk Markers in Type 2 Diabetes
- PMID: 38732624
- PMCID: PMC11085322
- DOI: 10.3390/nu16091378
The Impact of a Nutritional Intervention on Glycemic Control and Cardiovascular Risk Markers in Type 2 Diabetes
Abstract
Introduction: Nutritional management plays a crucial role in treating patients with type 2 diabetes (T2D), working to prevent and control the progression of chronic non-communicable diseases.
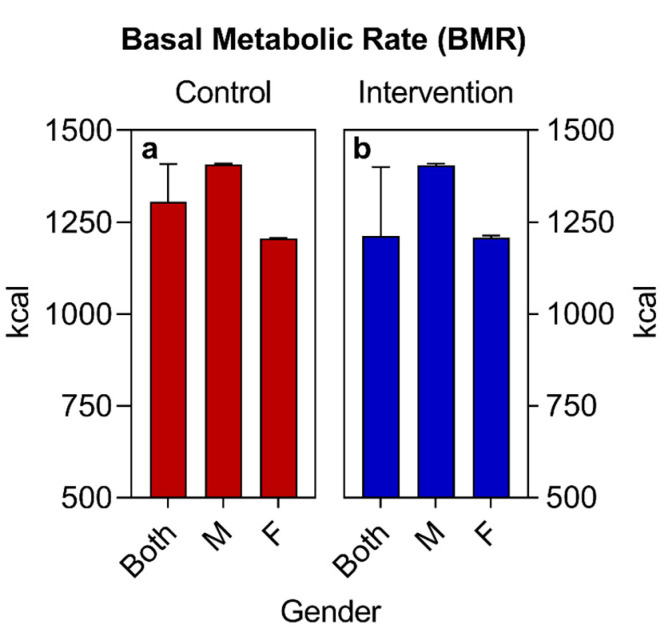
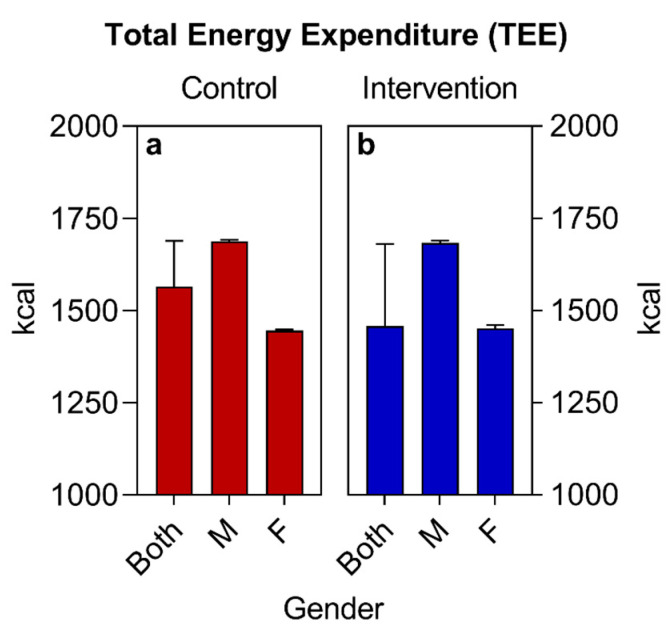
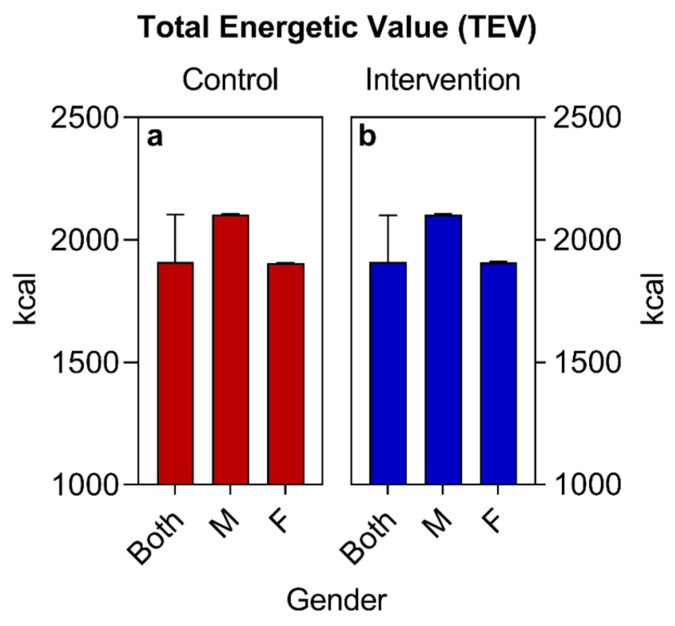
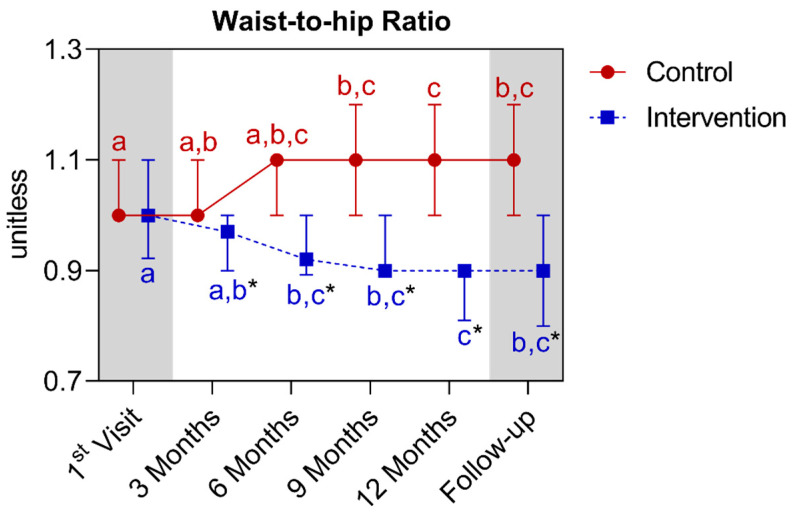
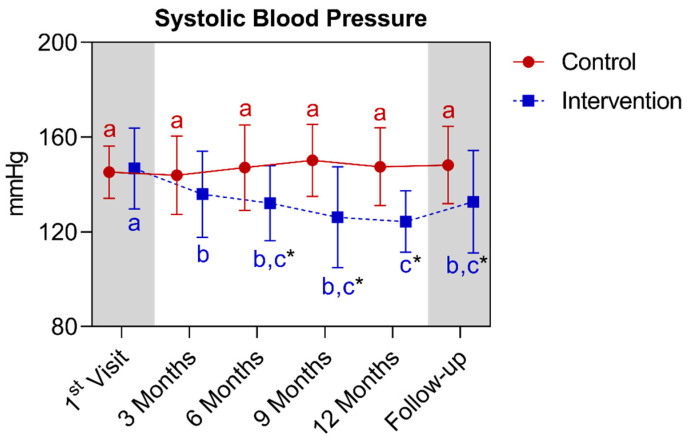
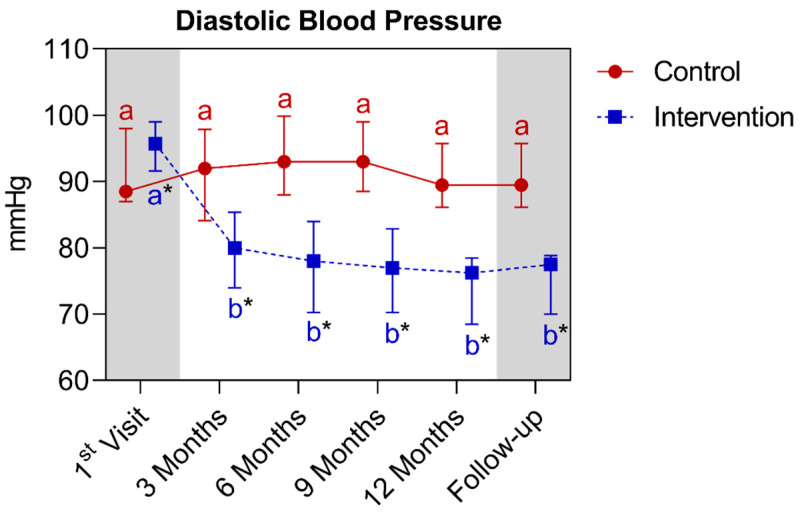
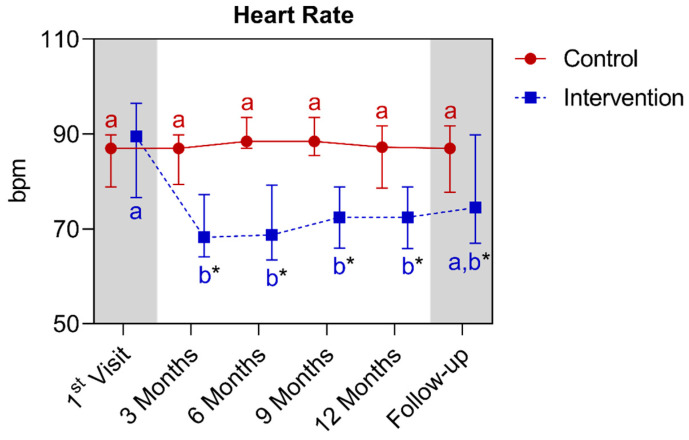
Objectives: To evaluate the effects of individualized nutritional interventions on weight, body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), fasting blood glucose (FBG), hemoglobin A1c (HbA1c), total cholesterol (TC), LDL cholesterol (LDL-C), HDL cholesterol (HDL-C), triglycerides (TGs), systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR)} over 12 months and subsequently at follow-up (15 months).
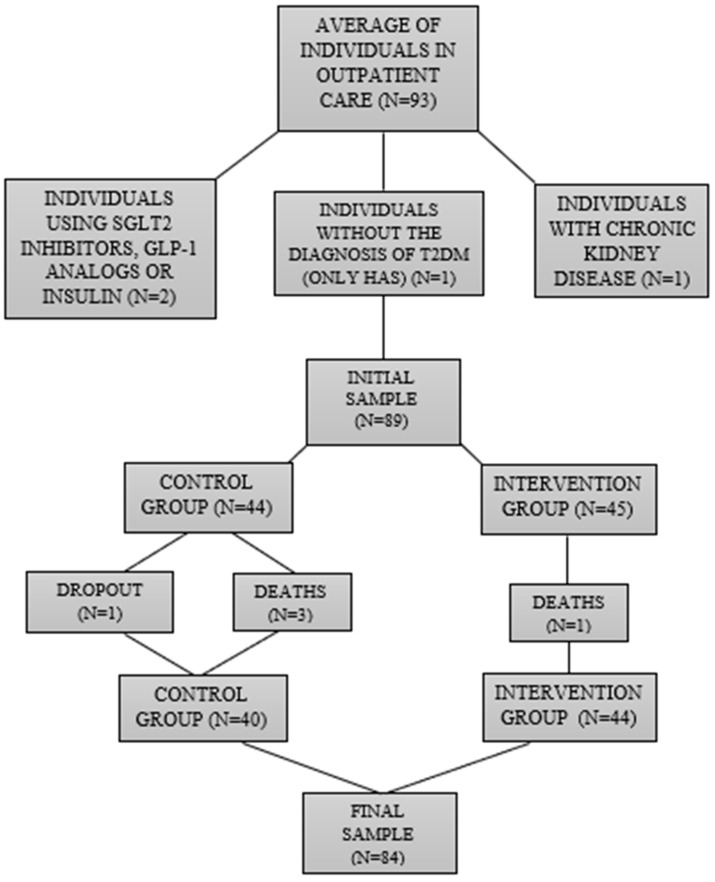
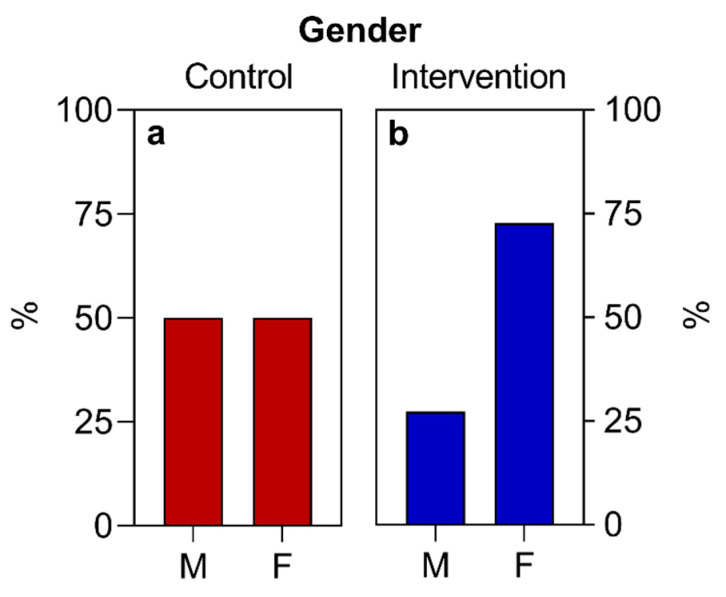
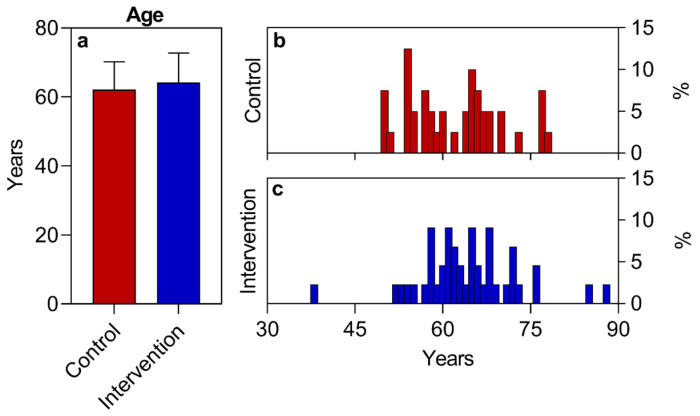
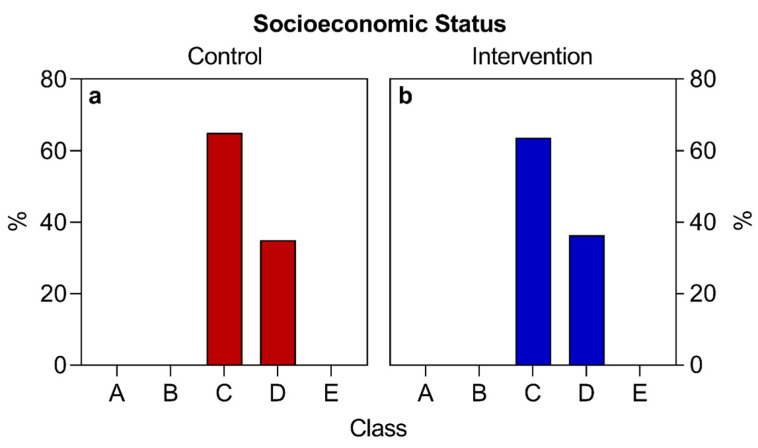
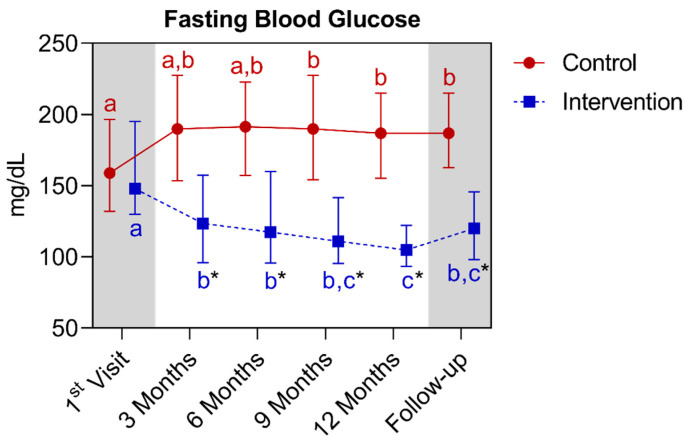
Methods: This longitudinal experimental study (without randomization and blinding) enrolled 84 sedentary participants with T2D (both sexes, aged 18-80 years). They were divided into a control group of 40 participants who received only medical consultations, and an intervention group of 44 participants who received the same medical care along with a nutritional assessment. Consultations occurred quarterly from August 2020 to November 2022 (first-twelfth month), with six to nine patients per session. Subsequently, a follow-up was conducted from December 2022 to November 2023, during which the intervention group had only medical care (during the 12th-15th months). Personalized dietary planning was inspired by the Mediterranean/DASH diets adapted to Brazilian foods and socioeconomic cultures.
Statistical analysis: Normal variables were compared between groups for each time point and also within each group across different time points using a two-way ANOVA (repeated measures for intragroup) followed by the Šídák post hoc test. Non-normal variables were compared between groups for each time point using Kruskal-Wallis followed by the Dunn post hoc test, and within each group across different time points using Friedman followed by the Dunn post hoc test. Data with a Gaussian distribution were presented as mean ± standard deviation (SD), and data with a non-Gaussian distribution were presented as median ± interquartile range (IQR). For all cases, α < 0.05 and p < 0.05 were adopted.
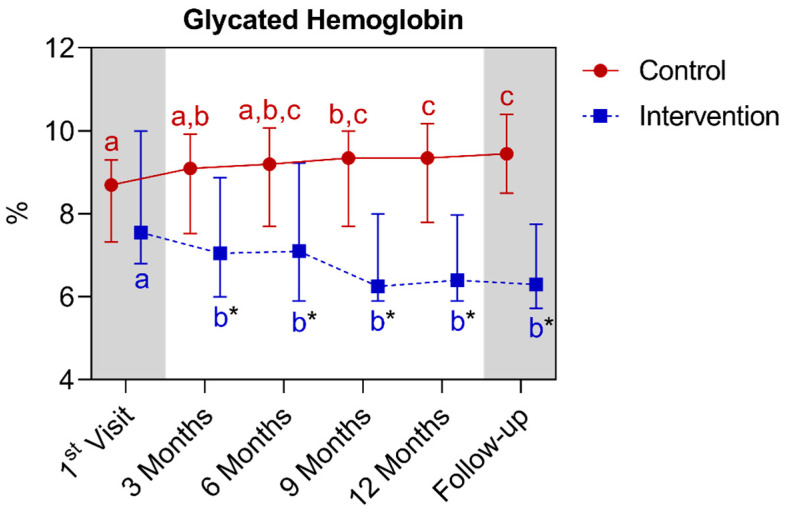
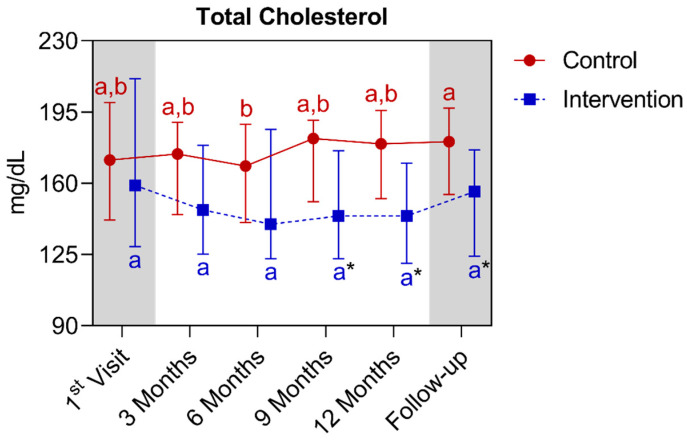
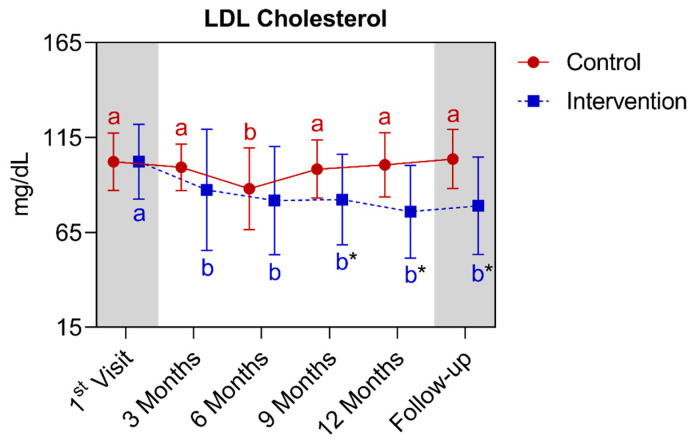
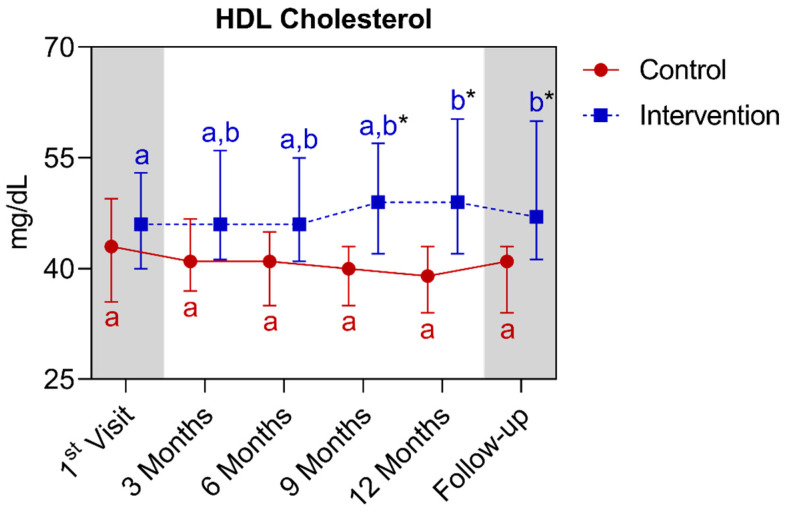
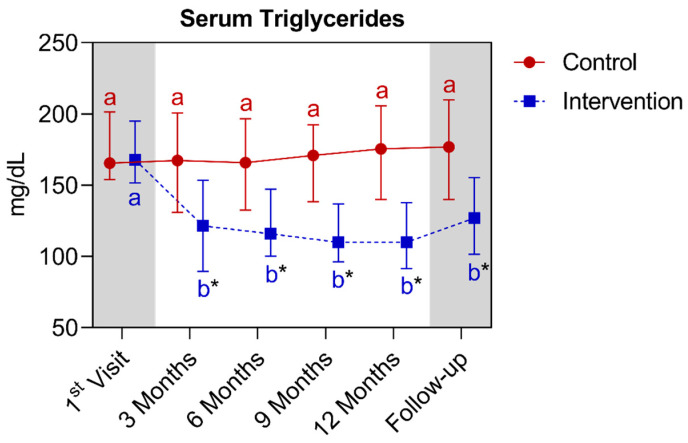
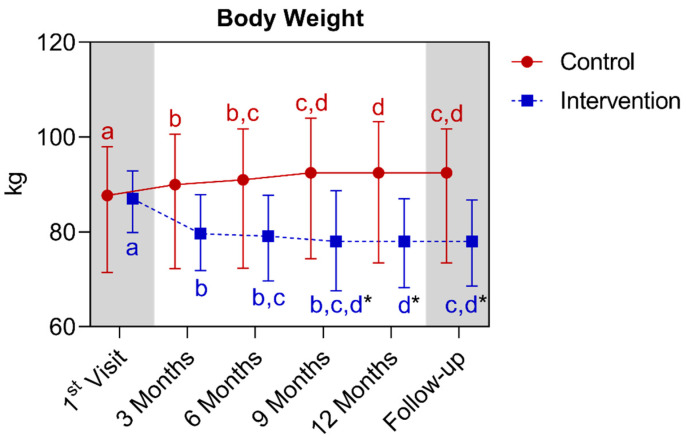
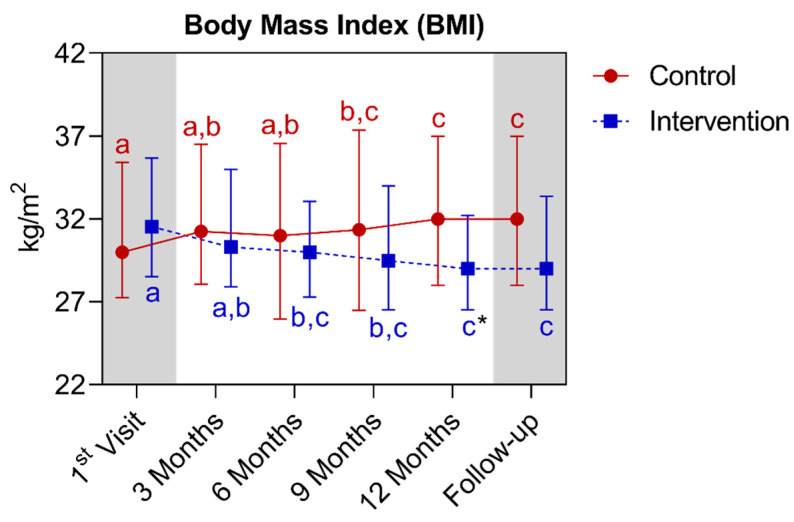
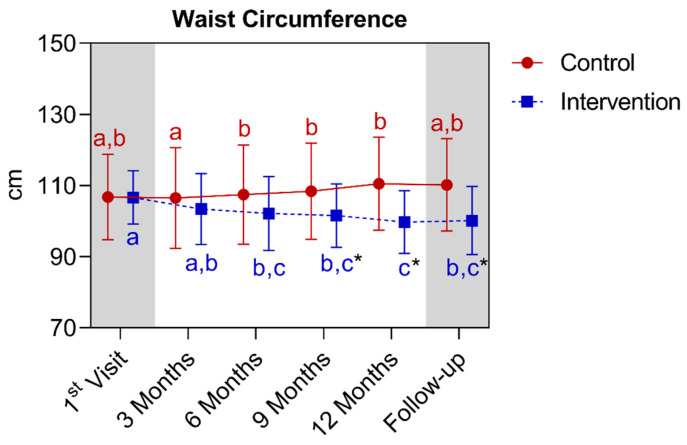
Results: In the intervention group, significant reductions were observed between the first and twelfth month for all parameters (p < 0.05), (except for TC), along with an increase in HDL-C (p = 0.0105). Conversely, in the control group, there was a significant increase in HbA1c, weight, BMI, FBG, and WHR (p < 0.05) between the first and twelfth months. Regarding the comparison between groups, there was a significant difference for all analyzed parameters (p < 0.05) from the first to the twelfth month. In the follow-up, differences were also observed (p < 0.05), except for BMI (p > 0.05).
Conclusion: The individualized nutritional intervention improved eating habits, anthropometric, biochemical, and cardiovascular markers in T2D over 12 months, with sustained results during follow-up. The dietary plan inspired by the Mediterranean and DASH diets demonstrated good adaptation to the Brazilian food culture and the patients' socioeconomic contexts. Consistent monitoring and personalized nutritional management are essential for optimizing long-term outcomes. However, more clinical trials are necessary in order to optimize the level of evidence for longitudinal interventions.
Keywords: DASH diet; HDL cholesterol; LDL cholesterol; Type 2 diabetes mellitus; blood glucose; blood pressure; cardiovascular risk markers; hemoglobin glycated; mediterranean diet; nutritional intervention; personalized nutrition; total cholesterol; triglycerides; weight.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- International Diabetes Federation . IDF Diabetes Atlas. 10th ed. International Diabetes Federation; Brussels, Belgium: 2021. [(accessed on 20 January 2022)]. Available online: http://www.diabetesatlas.org.
-
- ElSayed N.A., Aleppo G., Aroda V.R., Bannuru R.R., Brown F.M., Bruemmer D., Collins B.S., Hilliard M.E., Isaacs D., Johnson E.L., et al. 8. Association Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46((Suppl. S1)):S128–S139. doi: 10.2337/dc23-S008. - DOI - PMC - PubMed
-
- Marx N., Federici M., Schütt K., Müller-Wieland D., Ajjan R.A., Antunes M.J., Christodorescu R.M., Crawford C., Di Angelantonio E., Eliasson B., et al. ESC Scientific Document Group. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023;44:4043–4140. doi: 10.1093/eurheartj/ehad192. - DOI - PubMed
-
- World Health Organization (WHO) Fact Sheet: Obesity and Overweight. World Health Organization; Geneva, Switzerland: 2021. [(accessed on 20 November 2021)]. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- World Health Organization (WHO) Proposed Policy Priorities for Preventing Obesity and Diabetes in the Eastern Mediterranean Region. World Health Organization; Geneva, Switzerland: 2017. (Technical Report Series).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
