

Risk loci involved in giant cell arteritis susceptibility: a genome-wide association study
- PMID: 38734017
- PMCID: PMC11108802
- DOI: 10.1016/S2665-9913(24)00064-X
Risk loci involved in giant cell arteritis susceptibility: a genome-wide association study
Abstract
Background: Giant cell arteritis is an age-related vasculitis that mainly affects the aorta and its branches in individuals aged 50 years and older. Current options for diagnosis and treatment are scarce, highlighting the need to better understand its underlying pathogenesis. Genome-wide association studies (GWAS) have emerged as a powerful tool for unravelling the pathogenic mechanisms involved in complex diseases. We aimed to characterise the genetic basis of giant cell arteritis by performing the largest GWAS of this vasculitis to date and to assess the functional consequences and clinical implications of identified risk loci.
Methods: We collected and meta-analysed genomic data from patients with giant cell arteritis and healthy controls of European ancestry from ten cohorts across Europe and North America. Eligible patients required confirmation of giant cell arteritis diagnosis by positive temporal artery biopsy, positive temporal artery doppler ultrasonography, or imaging techniques confirming large-vessel vasculitis. We assessed the functional consequences of loci associated with giant cell arteritis using cell enrichment analysis, fine-mapping, and causal gene prioritisation. We also performed a drug repurposing analysis and developed a polygenic risk score to explore the clinical implications of our findings.
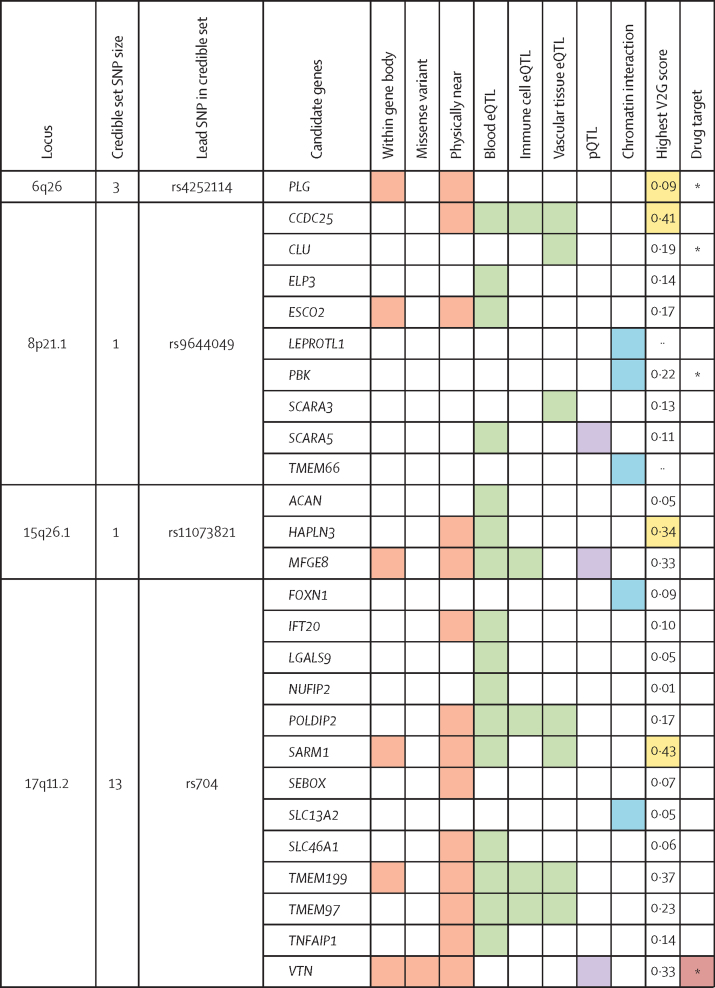
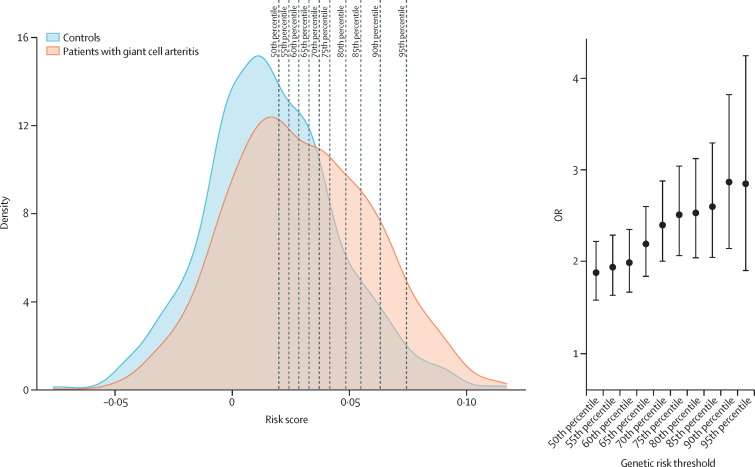
Findings: We included a total of 3498 patients with giant cell arteritis and 15 550 controls. We identified three novel loci associated with risk of giant cell arteritis. Two loci, MFGE8 (rs8029053; p=4·96 × 10-8; OR 1·19 [95% CI 1·12-1·26]) and VTN (rs704; p=2·75 × 10-9; OR 0·84 [0·79-0·89]), were related to angiogenesis pathways and the third locus, CCDC25 (rs11782624; p=1·28 × 10-8; OR 1·18 [1·12-1·25]), was related to neutrophil extracellular traps (NETs). We also found an association between this vasculitis and HLA region and PLG. Variants associated with giant cell arteritis seemed to fulfil a specific regulatory role in crucial immune cell types. Furthermore, we identified several drugs that could represent promising candidates for treatment of this disease. The polygenic risk score model was able to identify individuals at increased risk of developing giant cell arteritis (90th percentile OR 2·87 [95% CI 2·15-3·82]; p=1·73 × 10-13).
Interpretation: We have found several additional loci associated with giant cell arteritis, highlighting the crucial role of angiogenesis in disease susceptibility. Our study represents a step forward in the translation of genomic findings to clinical practice in giant cell arteritis, proposing new treatments and a method to measure genetic predisposition to this vasculitis.
Funding: Institute of Health Carlos III, Spanish Ministry of Science and Innovation, UK Medical Research Council, and National Institute for Health and Care Research.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MCC reports support from the Spanish Ministry of Science and Innovation (PID2020-114909RB-I00), Vasculitis Foundation, Agency for the Management of University and Research Grants (2021 SGR 01561), and Kiniksa Pharmaceuticals; consulting fees or honoraria from GSK, CSL Vifor, AbbVie, and AstraZeneca; support for attending meetings from Kiniksa Pharmaceuticals; and participation on a data safety monitoring board or advisory board for GSK, CSL Vifor, and AstraZeneca. GE has acted as a consultant for GSK, AstraZeneca, Sobi, Novartis, Boehringer, and CSL Vifor. AWM reports support from the UK Medical Research Council (MRC), National Institute for Health and Care Research (NIHR), Leeds Care, and Roche Products; and consulting fees or honoraria from CSL Vifor and AstraZeneca. PL reports grants or contracts from the Federal Ministry of Education and Research, German Research Society, German Society for Rheumatology, John Grube Foundation, and CSL Vifor; consulting fees or honoraria from GSK, CSL Vifor, AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Forum für medizinische Fortbildung, Janssen, Rheumaakademie, and UCB; support for attending meetings from CSL Vifor; and participation on a data safety monitoring board or advisory board for GSK, CSL Vifor, AbbVie, and Novartis. TW reports consulting fees or honoraria from AbbVie, AstraZeneca, Lilly, UCB, and Novartis; and participation on a data safety monitoring board or advisory board for AbbVie, AstraZeneca, Lilly, UCB, Novartis, and Fresenius. MAG-G reports honoraria from GSK. NK reports grants or contracts from Bristol Myers Squibb, AbbVie, and Sanofi; and consulting fees or honoraria from Roche, Otsuka, GSK, and Mallinckrodt. CAL reports grants or contracts from Bristol Myers Squibb and support from the National Institutes of Health. PAM reports grants, contracts, or consulting fees from AbbVie, Amgen, AstraZeneca, ArGenx, Boehringer Ingelheim, Bristol Myers Squibb, Cabaletta, CSL Behring, Eicos, Electra, Forbius, Genentech–Roche, GSK, HiBio, InflaRx, Janssen, Jubilant, Kyverna, MiroBio, Neutrolis, Novartis, NS Pharma, Q32, Regeneron, Sanofi, Sparrow, Takeda, and Vistera; royalties or licenses from UpToDate; and stock or stock options from Kyverna, Q32, and Sparrow. SLM reports grants or contracts from MRC, NIHR, and CSL Vifor; consulting fees from Roche, Sanofi, AbbVie, AstraZeneca, and Pfizer; payment or honoraria for lectures or educational events from Roche, Pfizer, UCB, CSL Vifor, Fresenius Kabi, and Novartis; support for attending meetings from Pfizer; participation on a data safety monitoring board or advisory board for Collaboration for Leadership in Applied Health Research and Care, Haywood Foundation, and GC-SheaLD; a leadership or fiduciary role in the British Society for Rheumatology Clinical Affairs Committee; participation as an investigator on industry-sponsored clinical trials for Sanofi; and infrastructure support from MRC. LB reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Instrumentation Laboratory SPA and AbbVie; and support for attending meetings from AbbVie and Novartis. EB reports payments or honoraria from EULAR and received grants from the Dutch Arthritis Society DAS and the EU/EFPIA/Innovative Medicines Initiative 2 Joint Undertaking Immune-Image grant no 831514. EB is member of the board of the non-profit organisation, Auto-immune Research Hub, in the Netherlands. All other authors declare no competing interests.
Figures
References
-
- Ciccia F, Rizzo A, Ferrante A, et al. New insights into the pathogenesis of giant cell arteritis. Autoimmun Rev. 2017;16:675–683. - PubMed
-
- Tomelleri A, van der Geest KSM, Khurshid MA, et al. Disease stratification in GCA and PMR: state of the art and future perspectives. Nat Rev Rheumatol. 2023;19:446–459. - PubMed
-
- Ortíz-Fernández L, Martín J, Alarcón-Riquelme ME. A summary on the genetics of systemic lupus erythematosus, rheumatoid arthritis, systemic sclerosis, and Sjögren's syndrome. Clin Rev Allergy Immunol. 2023;64:392–411. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
