

Baseline and end-of-treatment host serum biomarkers predict relapse in adults with pulmonary tuberculosis
- PMID: 38734311
- PMCID: PMC11180560
- DOI: 10.1016/j.jinf.2024.106173
Baseline and end-of-treatment host serum biomarkers predict relapse in adults with pulmonary tuberculosis
Abstract
Background: There is a need for new tools for monitoring of the response to TB treatment. Such tools may allow for tailored treatment regimens, and stratify patients initiating TB treatment into different risk groups. We evaluated combinations between previously published host biomarkers and new candidates, as tools for monitoring TB treatment response, and prediction of relapse.
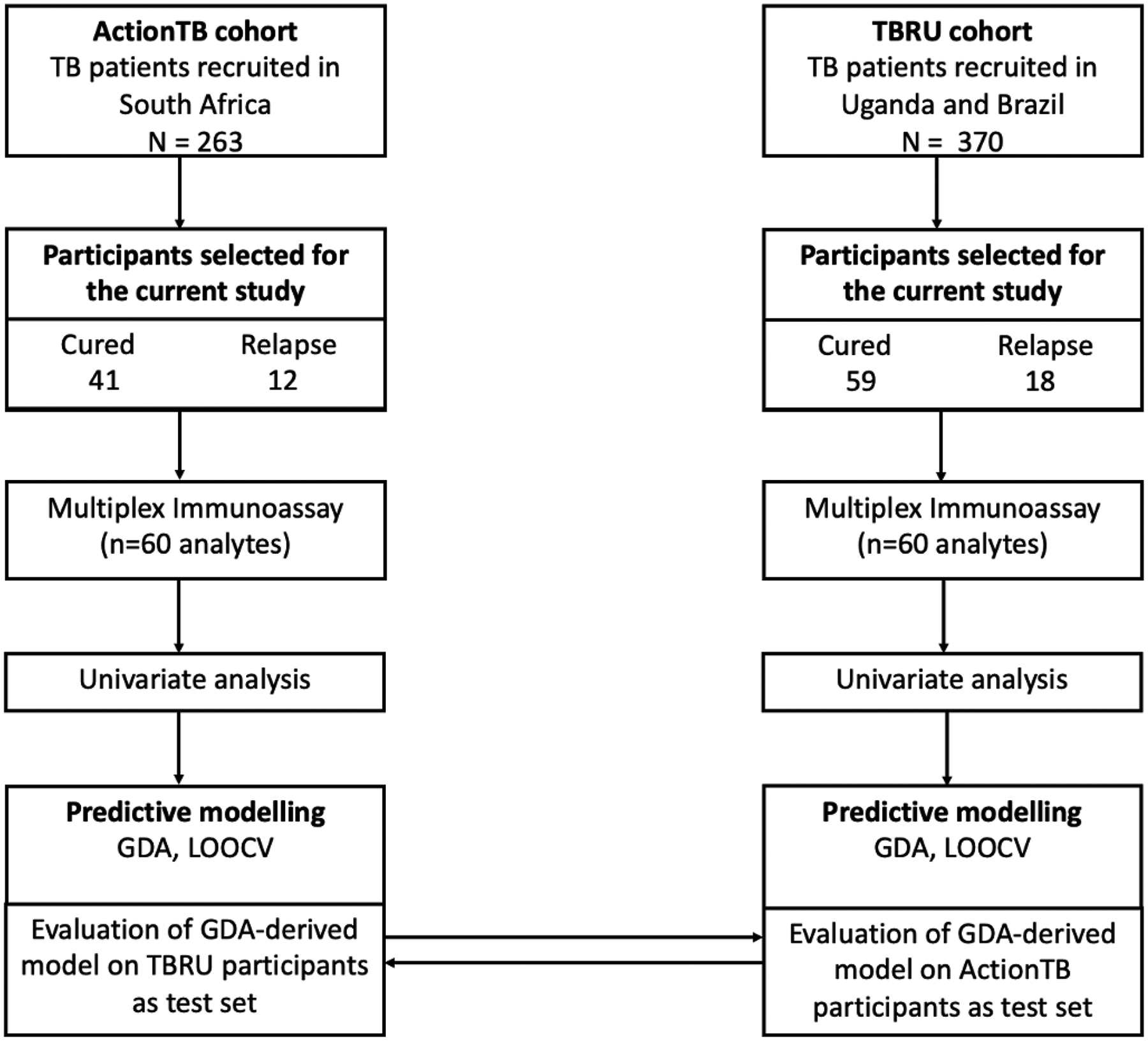
Methods: Serum samples were collected at multiple time points, from patients initiating TB treatment at research sites situated in South Africa (ActionTB study), Brazil and Uganda (TBRU study). Using a multiplex immunoassay platform, we evaluated the concentrations of selected host inflammatory biomarkers in sera obtained from clinically cured patients with and without subsequent relapse within 2 years of TB treatment completion.
Results: A total of 130 TB patients, 30 (23%) of whom had confirmed relapse were included in the study. The median time to relapse was 9.7 months in the ActionTB study (n = 12 patients who relapsed), and 5 months (n = 18 patients who relapsed) in the TBRU study. Serum concentrations of several host biomarkers changed during TB treatment with IL-6, IP-10, IL-22 and complement C3 showing potential individually, in predicting relapse. A six-marker signature comprising of TTP, BMI, sICAM-1, IL-22, IL-1β and complement C3, predicted relapse, prior to the onset of TB treatment with 89% sensitivity and 94% specificity. Furthermore, a 3-marker signature (Apo-CIII, IP-10 and sIL-6R) predicted relapse in samples collected at the end of TB treatment with sensitivity of 71% and specificity of 74%. A previously identified baseline relapse prediction signature (TTP, BMI, TNF-β, sIL-6R, IL-12p40 and IP-10) also showed potential in the current study.
Conclusion: Serum host inflammatory biomarkers may be useful in predicting relapse in TB patients prior to the initiation of treatment. Our findings have implications for tailored patient management and require prospective evaluation in larger studies.
Keywords: Biomarkers; Biosignatures; Relapse; Treatment response; Tuberculosis.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Global tuberculosis report 2023. Accessed March 14, 2024. https://www.who.int/publications/i/item/9789240083851
-
- Organization WH. Treatment of Tuberculosis: Guidelines. World Health Organization; 2010. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
