

Positive resection margins in Crohn's disease are a relevant risk factor for postoperative disease recurrence
- PMID: 38734721
- PMCID: PMC11088694
- DOI: 10.1038/s41598-024-61697-w
Positive resection margins in Crohn's disease are a relevant risk factor for postoperative disease recurrence
Abstract
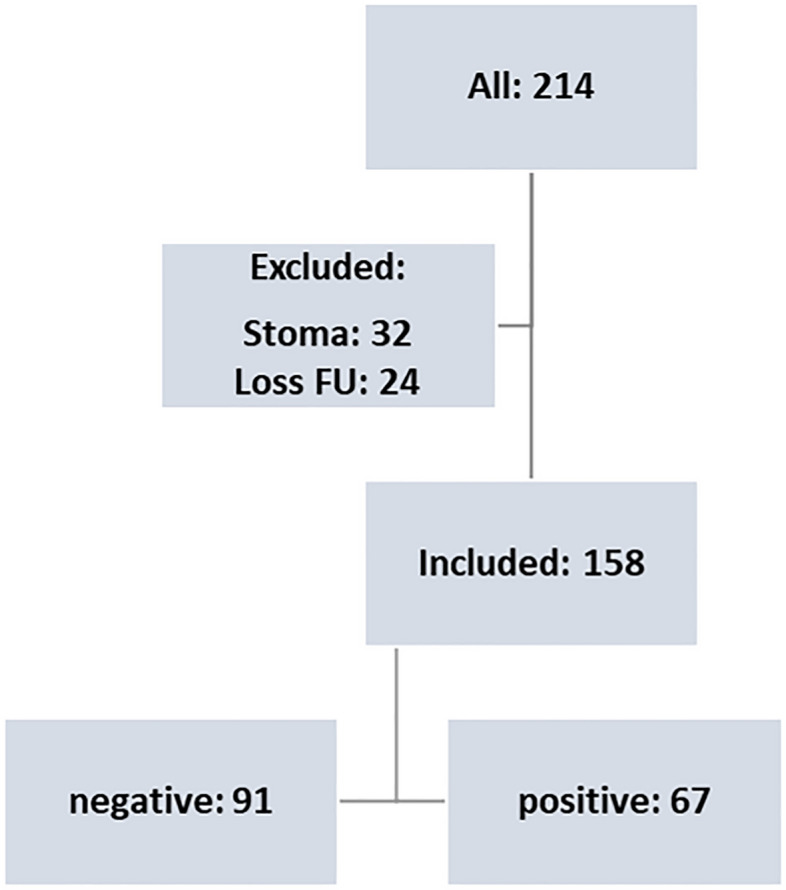
Postoperative disease recurrence in Crohn's disease represents a relevant issue despite recent advancements in surgical and medical therapies. Additional criteria are necessary to improve the identification of patients at risk and to enable selective therapeutic approaches. The role of resection margins on disease recurrence remains unclear and general recommendations are lacking. A single-center retrospective analysis was performed including all patients who received ileocecal resection due to Crohn's disease. Resection margins were analyzed by two independent pathologists and defined by histopathological criteria based on previous consensus reports. 158 patients were included for analysis with a median follow up of 35 months. While postoperative morbidity was not affected, positive resection margins resulted in significantly increased rates of severe endoscopic recurrence at 6 months (2.0% versus 15.6%, p = 0.02) and overall (4.2% versus 19.6%, p = 0.001), which resulted in significantly increased numbers of surgical recurrence (0% versus 4.5%, p = 0.04). Additionally, positive margins were identified as independent risk factor for severe endoscopic disease recurrence in a multivariate analysis. Based on that, positive margins represent an independent risk factor for postoperative endoscopic and surgical disease recurrence. Prospective studies are required to determine whether extended resection or postoperative medical prophylaxis is beneficial for patients with positive resection margins.
Keywords: Crohn’s disease; Ileocecal resection; Postoperative disease recurrence.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Murthy SK, Begum J, Benchimol EI, Bernstein CN, Kaplan GG, McCurdy JD, et al. Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: A population-based interrupted time series study. Gut. 2020;69(2):274–282. doi: 10.1136/gutjnl-2019-318440. - DOI - PMC - PubMed
-
- Ponsioen CY, de Groof EJ, Eshuis EJ, Gardenbroek TJ, Bossuyt PMM, Hart A, et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: A randomised controlled, open-label, multicentre trial. Lancet Gastroenterol. Hepatol. 2017;2(11):785–792. doi: 10.1016/S2468-1253(17)30248-0. - DOI - PubMed
-
- Stevens TW, Haasnoot ML, D'Haens GR, Buskens CJ, de Groof EJ, Eshuis EJ, et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: Retrospective long-term follow-up of the LIR!C trial. Lancet Gastroenterol. Hepatol. 2020;5(10):900–907. doi: 10.1016/S2468-1253(20)30117-5. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
