

Primary hyperoxaluria in adults and children: a nationwide cohort highlights a persistent diagnostic delay
- PMID: 38737343
- PMCID: PMC11087826
- DOI: 10.1093/ckj/sfae099
Primary hyperoxaluria in adults and children: a nationwide cohort highlights a persistent diagnostic delay
Abstract
Background: Primary hyperoxalurias (PH) are extremely rare genetic disorders characterized by clinical heterogeneity. Delay in diagnosing these conditions can have detrimental effects on patient outcomes. The primary objective of this study is to assess the current diagnostic delay for PH.
Methods: This nationwide, observational and retrospective study included patients who received a genetic diagnosis of PH types 1, 2 and 3 between 1 January 2015 and 31 December 2019. Diagnostic delay was defined as the duration between the onset of symptoms and the time of genetic diagnosis.
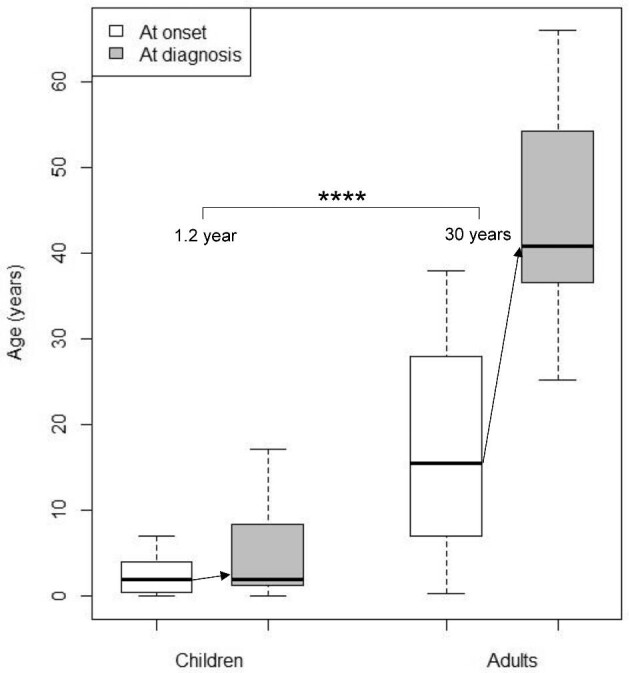
Results: A total of 52 patients (34 children and 18 adults) were included in the study, with 40 PH1 (77%), 3 PH2 (6%) and 9 PH3 (17%). At the time of diagnosis, 12 patients (23%) required dialysis. Among the PH1 patients, the predominant symptom at onset in adults was renal colic (79% of cases), whereas symptoms in children were more diverse (renal colic in 17% of cases). The diagnostic delay was significantly shorter in children compared with adults [median (interquartile range)]: 1.2 (0.1-3.0) versus 30 (17-36) years, respectively (P < .0001). RNA interference was utilized in 23 patients (58%). Five individuals (13%) underwent double liver-kidney transplantation, and five (13%) received isolated kidney transplantation, with lumasiran therapy in four patients. For PH2 and PH3 patients, the diagnostic delay ranges from 0 to 3 years, with renal colic as first symptom in 33% of cases.
Conclusion: This extensive and recent cohort of PH underscores the considerable delay in diagnosing PH, particularly in adults, even in a country with a dedicated organization for enhancing the overall management of rare diseases. These findings reinforce the imperative for increased awareness among relevant specialties regarding the evaluation of urolithiasis.
Keywords: diagnostic delay; genetic testing; nephrolithiasis; orphan disease; primary hyperoxaluria.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
R.P. received funding from Alnylam Pharmaceuticals to attend a national nephrology congress. C.A. received consulting fees for Alnylam and Novonordisk. N.B. received help for medical writing from Alnylam. S.B. received fees from AstraZeneca, Lilly, CSL Vifor, Bayer and IKI. I.B., K.C., C.D., M.G., F.H. and C.R.-R. declare no conflict of interest. E.L. patented Stiripentol to reduce urine oxalate excretion (WO2017140658A1) and received consulting fees from Biocodex Laboratory. J.B. received travel, consulting and speaker fees from Alnylam Pharmaceuticals, and consulting fees from Dicenra/Novonordisk Pharmaceuticals and Biocodex Pharmaceuticals. B.M. received consulting, travel and speaker fees from Alnylam Pharmaceuticals.
Figures

References
-
- Bouzidi H, Majdoub A, Daudon M et al. Hyperoxalurie primitive : une revue de la littérature. Nephrol Ther 2016;12:431–6. - PubMed
LinkOut - more resources
Full Text Sources
