

Evolution of invasive pneumococcal disease by serotype 3 in adults: a Spanish three-decade retrospective study
- PMID: 38737571
- PMCID: PMC11087702
- DOI: 10.1016/j.lanepe.2024.100913
Evolution of invasive pneumococcal disease by serotype 3 in adults: a Spanish three-decade retrospective study
Abstract
Background: Invasive pneumococcal disease due to serotype 3 (S3-IPD) is associated with high mortality rates and long-term adverse effects. The introduction of the 13-valent pneumococcal conjugate vaccine (PCV13) into the Spanish paediatric immunisation programme has not led to a decrease in the adult S3-IPD. We aimed to analyse the incidence, clinical characteristics and genomics of S3-IPD in adults in Spain.
Methods: Adult IPD episodes hospitalized in a Southern Barcelona hospital were prospectively collected (1994-2020). For genomic comparison, S3-IPD isolates from six Spanish hospitals (2008-2020) and historical isolates (1989-1993) were analysed by WGS (Illumina and/or MinION).
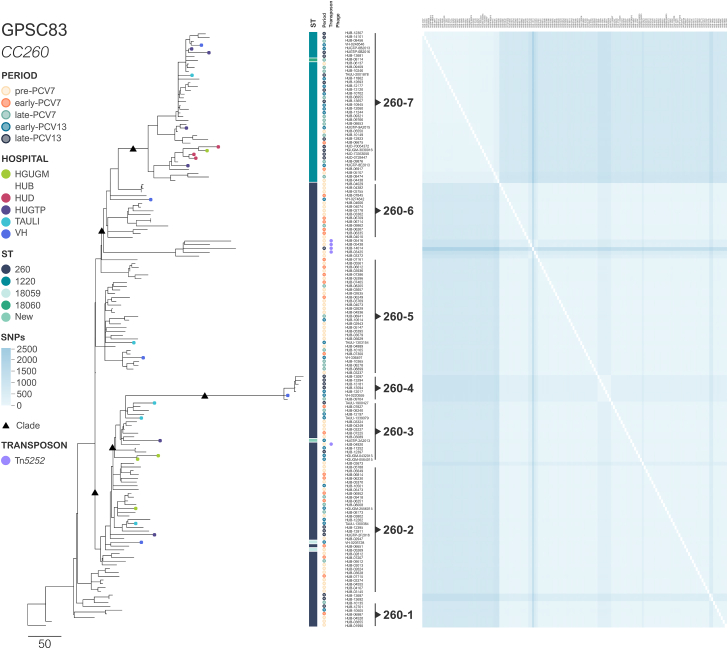
Findings: From 1994 to 2020, 270 S3-IPD episodes were detected. When comparing pre-PCV (1994-2001) and late-PCV13 (2016-2020) periods, only modest changes in S3-IPD were observed (from 1.58 to 1.28 episodes per 100,000 inhabitants year). In this period, the incidence of the two main lineages shifted from 0.38 to 0.67 (CC180-GPSC12) and from 1.18 to 0.55 (CC260-GPSC83). The overall 30-day mortality remained high (24.1%), though a decrease was observed between the pre-PCV (32.4%; 95.0% CI, 22.0-45.0) and the late-PCV13 period (16.7%; 95.0% CI, 7.5-32.0) (p = 0.06). At the same time, comorbidities increased from 77.3% (95.0% CI, 65.0-86.0) to 85.7% (95.0% CI, 71.0-94.0) (p = 0.69). There were no differences in clinical characteristics or 30-day mortality between the two S3 lineages. Although both lineages were genetically homogeneous, the CC180-GPSC12 lineage presented a higher SNP density, a more open pan-genome, and a major presence of prophages and mobile genetic elements carrying resistance genes.
Interpretation: Adult S3-IPD remained stable in our area over the study period despite PCV13 introduction in children. However, a clonal shift was observed. The decrease in mortality rates and the increase in comorbidities suggest a change in clinical management and overall population characteristics. The low genetic variability and absence of clinical differences between lineages highlight the role of the S3 capsule in the disease severity.
Funding: This study has been funded by Instituto de Salud Carlos III (ISCIII) "PI18/00339", "PI21/01000", "INT22/00096", "FI22/00279", CIBER "CIBERES-CB06/06/0037", "CIBERINFEC-CB21/13/00009" and MSD grant "IISP 60168".
Keywords: Genomics; Serotype 3; Streptococcus pneumoniae.
© 2024 The Author(s).
Conflict of interest statement
C.A. has been a scientific adviser for, and/or has received research funding from, Merck Sharp & Dohme Corp and Pfizer. J.Y. has been a scientific adviser for, and/or has received research funding from, Merck Sharp & Dohme Corp, Pfizer and GSK. All other authors declare that they have no conflicts of interest regarding this research.
Figures



References
-
- Grau I., Ardanuy C., Cubero M., et al. Declining mortality from adult pneumococcal infections linked to children's vaccination. J Infect. 2016;72:439–449. - PubMed
-
- Garcia-Vidal C., Ardanuy C., Tubau F., et al. Pneumococcal pneumonia presenting with septic shock: host- and pathogen-related factors and outcomes. Thorax. 2010;65:77–81. - PubMed
LinkOut - more resources
Full Text Sources
