

Preemptive treatment in the acute and early subacute phase of uncomplicated type B aortic dissections with poor prognosis factors
- PMID: 38737713
- PMCID: PMC11082266
- DOI: 10.3389/fcvm.2024.1362576
Preemptive treatment in the acute and early subacute phase of uncomplicated type B aortic dissections with poor prognosis factors
Abstract
Objective: Due to its favorable outcome regarding late morbidity and mortality, thoracic endovascular repair (TEVAR) is becoming more popular for uncomplicated type B aortic dissection (TBAD). This study aimed to compare preemptive endovascular treatment and optimal medical treatment (OMT) and OMT alone in patients presenting uncomplicated TBAD with predictors of aortic progression.
Design: Retrospective multicenter study.
Methods: We analyzed patients with uncomplicated TBAD and risk factors of progression in two French academic centers. Aortic events [defined as aortic-related (re)intervention or aortic-related death after initial hospitalization], postoperative complications, non-aortic events, and radiologic aortic progression and remodeling were recorded and analyzed. Analysis was performed on an intention-to-treat basis.
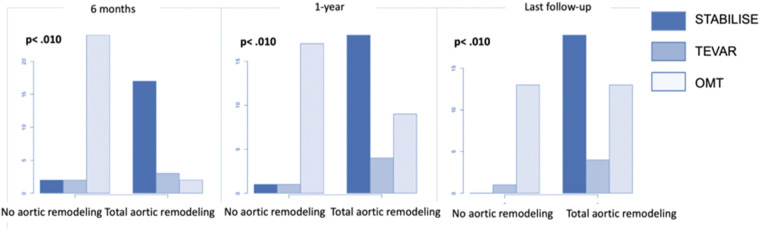
Results: Between 2011 and 2021, preemptive endovascular procedures at the acute and early subacute phase (<30 days) were performed on 24 patients (group 1) and OMT alone on 26 patients (group 2). With a mean follow-up of 38.08 ± 24.53 months, aortic events occurred in 20.83% of patients from group 1 and 61.54% of patients from group 2 (p < .001). No patient presented aortic-related death during follow-up. There were no differences in postoperative events (p = 1.00) and non-aortic events (p = 1.00). OMT patients had significantly more aneurysmal progression of the thoracic aorta (p < .001) and maximal aortic diameter (p < .001). Aortic remodeling was found in 91.67% of patients in group 1 and 42.31% of patients in group 2 (p < .001). A subgroup analysis of patients in group 1 showed that patients treated with preemptive TEVAR and STABILISE had reduced maximum aortic diameters at the 1-year (p = .010) and last follow-up (p = .030) compared to those in patients treated with preemptive TEVAR alone.
Conclusion: Preemptive treatment of uncomplicated TBAD with risk factors of progression reduces the risk of long-term aortic events. Over 60% of medically treated patients will require intervention during follow-up, with no benefit in terms of postoperative events. Even after surgical treatment, patients in the OMT group had significantly more aneurysmal progression, along with poorer aortic remodeling.
Keywords: aneurysmal evolution; comparative study; optimal medical treatment; preemptive endovascular treatment; risk factors; uncomplicated type B aortic dissection.
© 2024 Sachs, Vecchini, Corniquet, Bartoli, Barral, De Masi, Omnes, Piquet, Alsac and Gaudry.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Nienaber CA, Kische S, Rousseau H, Eggebrecht H, Rehders TC, Kundt G, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ: Cardiovasc Interv. (2013) 6(4):407–16. 10.1161/CIRCINTERVENTIONS.113.000463 - DOI - PubMed
LinkOut - more resources
Full Text Sources