

Acupuncture for Chronic Radiation-Induced Xerostomia in Head and Neck Cancer: A Multicenter Randomized Clinical Trial
- PMID: 38739392
- PMCID: PMC11091764
- DOI: 10.1001/jamanetworkopen.2024.10421
Acupuncture for Chronic Radiation-Induced Xerostomia in Head and Neck Cancer: A Multicenter Randomized Clinical Trial
Abstract
Importance: Patients with head and neck cancer who undergo radiotherapy can develop chronic radiation-induced xerostomia. Prior acupuncture studies were single center and rated as having high risk of bias, making it difficult to know the benefits of acupuncture for treating radiation-induced xerostomia.
Objective: To compare true acupuncture (TA), sham acupuncture (SA), and standard oral hygiene (SOH) for treating radiation-induced xerostomia.
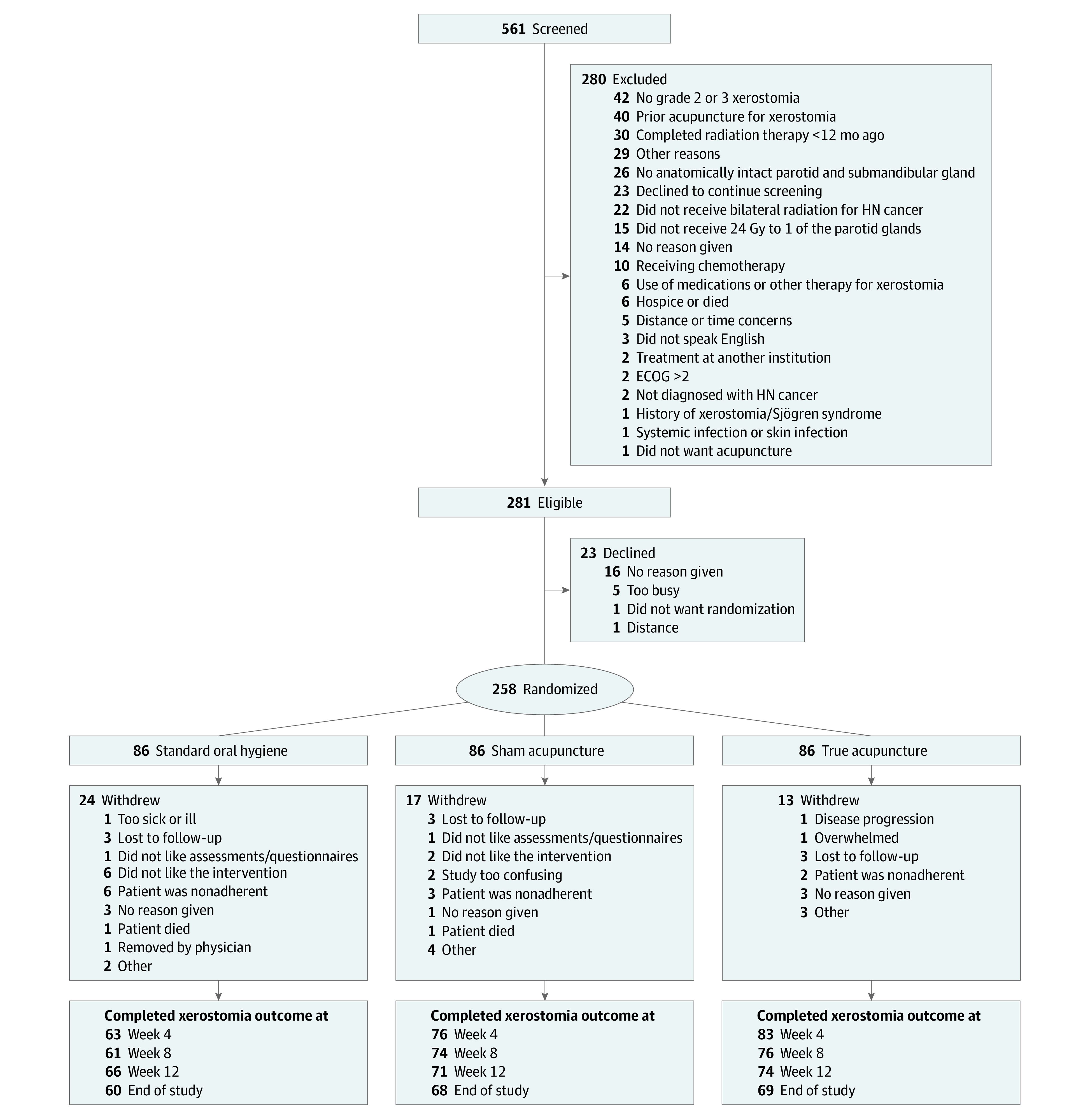
Design, setting, and participants: A randomized, blinded, 3-arm, placebo-controlled trial was conducted between July 29, 2013, and June 9, 2021. Data analysis was performed from March 9, 2022, through May 17, 2023. Patients reporting grade 2 or 3 radiation-induced xerostomia 12 months or more postradiotherapy for head and neck cancer were recruited from community-based cancer centers across the US that were part of the Wake Forest National Cancer Institute Community Oncology Research Program Research Base. Participants had received bilateral radiotherapy with no history of xerostomia.
Interventions: Participants received SOH and were randomized to TA, SA, or SOH only. Participants in the TA and SA cohorts were treated 2 times per week for 4 weeks. Those experiencing a minor response received another 4 weeks of treatment.
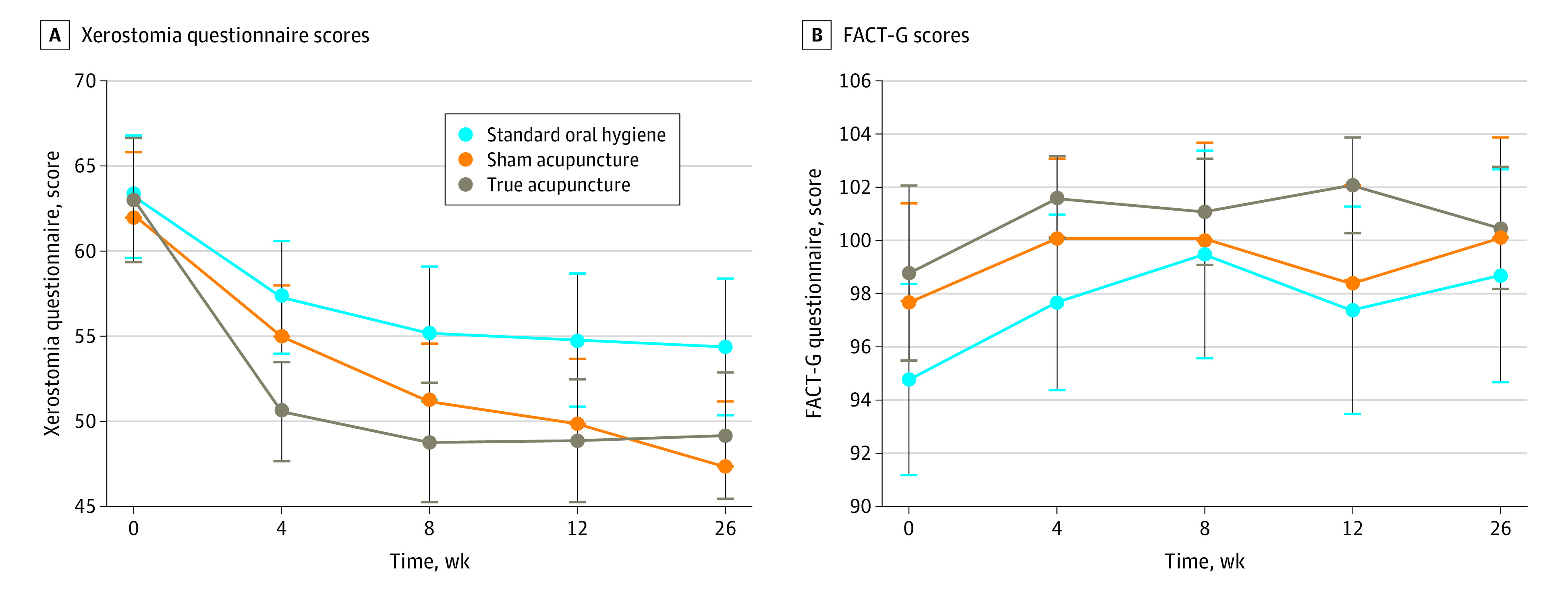
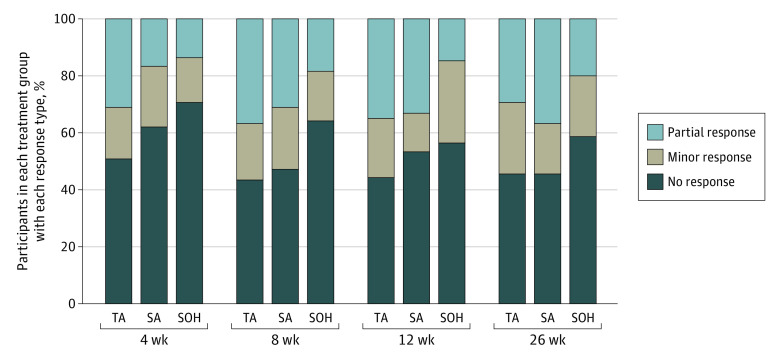
Main outcomes and measures: Patient-reported outcomes for xerostomia (Xerostomia Questionnaire, primary outcome) and quality of life (Functional Assessment of Cancer Therapy-General) were collected at baseline, 4 (primary time point), 8, 12, and 26 weeks. All analyses were intention to treat.
Results: A total of 258 patients (201 men [77.9%]; mean [SD] age, 65.0 [9.16] years), participated from 33 sites across 13 states. Overall, 86 patients were assigned to each study arm. Mean (SD) years from diagnosis was 4.21 (3.74) years, 67.1% (n = 173) had stage IV disease. At week 4, Xerostomia Questionnaire scores revealed significant between-group differences, with lower Xerostomia Questionnaire scores with TA vs SOH (TA: 50.6; SOH: 57.3; difference, -6.67; 95% CI, -11.08 to -2.27; P = .003), and differences between TA and SA (TA: 50.6; SA: 55.0; difference, -4.41; 95% CI, -8.62 to -0.19; P = .04) yet did not reach statistical significance after adjustment for multiple comparisons. There was no significant difference between SA and SOH. Group differences in Functional Assessment of Cancer Therapy-General scores revealed statistically significant group differences at week 4, with higher scores with TA vs SOH (TA: 101.6; SOH: 97.7; difference, 3.91; 95% CI, 1.43-6.38; P = .002) and at week 12, with higher scores with TA vs SA (TA: 102.1; SA: 98.4; difference, 3.64; 95% CI, 1.10-6.18; P = .005) and TA vs SOH (TA: 102.1; SOH: 97.4; difference, 4.61; 95% CI, 1.99-7.23; P = .001).
Conclusions and relevance: The findings of this trial suggest that TA was more effective in treating chronic radiation-induced xerostomia 1 or more years after the end of radiotherapy than SA or SOH.
Trial registration: ClinicalTrials.gov Identifier: NCT02589938.
Conflict of interest statement
Figures
References
-
- Eisbruch A, Ten Haken RK, Kim HM, Marsh LH, Ship JA. Dose, volume, and function relationships in parotid salivary glands following conformal and intensity-modulated irradiation of head and neck cancer. Int J Radiat Oncol Biol Phys. 1999;45(3):577-587. doi:10.1016/S0360-3016(99)00247-3 - DOI - PubMed
-
- Bertram U. Xerostomia: clinical aspects, pathology and pathogenesis. Acta Odontol Scand. 1967;25(suppl 49):e2410421. - PubMed
