

Assessment of Spillover of Antimicrobial Resistance to Untreated Children 7-12 Years Old After Mass Drug Administration of Azithromycin for Child Survival in Niger: A Secondary Analysis of the MORDOR Cluster-Randomized Trial
- PMID: 38739754
- PMCID: PMC11581702
- DOI: 10.1093/cid/ciae267
Assessment of Spillover of Antimicrobial Resistance to Untreated Children 7-12 Years Old After Mass Drug Administration of Azithromycin for Child Survival in Niger: A Secondary Analysis of the MORDOR Cluster-Randomized Trial
Abstract
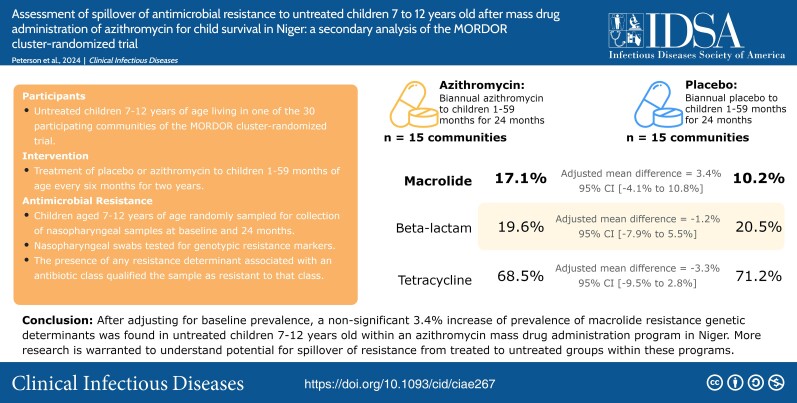
Background: The risk of antibiotic resistance is complicated by the potential for spillover effects from one treated population to another. Azithromycin mass drug administration programs report higher rates of antibiotic resistance among treatment arms in targeted groups. This study aimed to understand the risk of spillover of antibiotic resistance to nontarget groups in these programs.
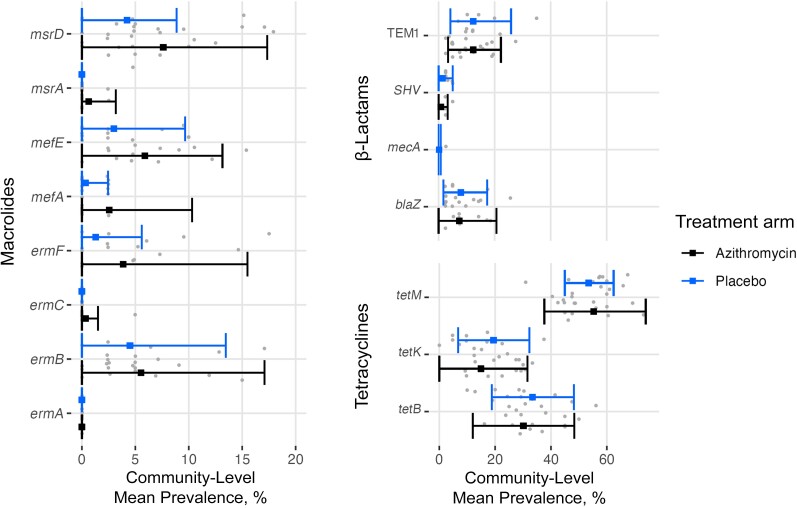
Methods: Data were used from a cluster-randomized trial comparing the effects of biannual azithromycin and placebo distribution to children 1-59 months old on child mortality rates. Nasopharyngeal samples from untreated children 7-12 years old were tested for genetic determinants of macrolide resistance (primary outcome) and resistance to other antibiotic classes (secondary outcomes). Linear regression was used to compare the community-level mean difference in prevalence by arm at the 24-month time point, adjusting for baseline prevalence.
Results: A total of 1103 children 7-12 years old in 30 communities were included in the analysis (15 azithromycin, 15 placebo). The adjusted mean differences in the prevalence of resistance determinants for macrolides, β-lactams, and tetracyclines were 3.4% (95% confidence interval, -4.1% to 10.8%; P = .37), -1.2% (-7.9% to 5.5%; P = .72), and -3.3% (-9.5% to 2.8%; P = .61), respectively.
Conclusions: We were unable to demonstrate a statistically significant increase in macrolide resistance determinants in untreated groups in an azithromycin mass drug administration program. While the result might be consistent with a small spillover effect, this study was not powered to detect such a small difference. Larger studies are warranted to better quantify the potential for spillover effects within these programs.
Trial registration: ClinicalTrials.gov NCT02047981.
Keywords: Niger; antimicrobial resistance; azithromycin; mass drug administration; spillover.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Figures


References
-
- Gottesman BS, Low M, Almog R, Chowers M. Quinolone consumption by mothers increases their children's risk of acquiring quinolone-resistant bacteriuria. Clin Infect Dis 2020; 71:532–8. - PubMed
-
- Samore MH, Magill MK, Alder SC, et al. High rates of multiple antibiotic resistance in Streptococcus pneumoniae from healthy children living in isolated rural communities: association with cephalosporin use and intrafamilial transmission 2001. Available at: http://publications.aap.org/pediatrics/article-pdf/108/4/856/894479/pe10.... Accessed 14 July 2023. - PubMed
