

Unveiling the oral-gut connection: chronic apical periodontitis accelerates atherosclerosis via gut microbiota dysbiosis and altered metabolites in apoE-/- Mice on a high-fat diet
- PMID: 38740741
- PMCID: PMC11091127
- DOI: 10.1038/s41368-024-00301-3
Unveiling the oral-gut connection: chronic apical periodontitis accelerates atherosclerosis via gut microbiota dysbiosis and altered metabolites in apoE-/- Mice on a high-fat diet
Abstract
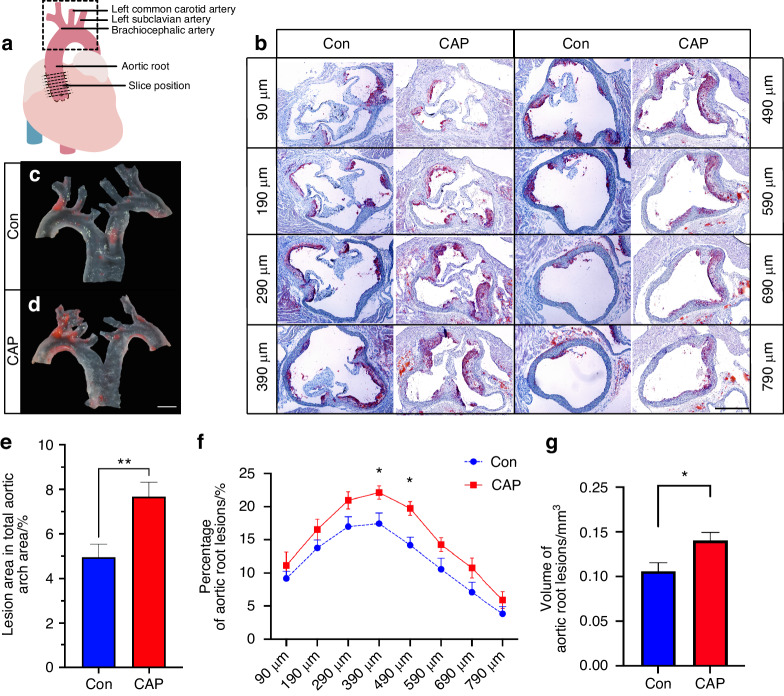
The aim of this study was to explore the impact of chronic apical periodontitis (CAP) on atherosclerosis in apoE-/- mice fed high-fat diet (HFD). This investigation focused on the gut microbiota, metabolites, and intestinal barrier function to uncover potential links between oral health and cardiovascular disease (CVD). In this study, CAP was shown to exacerbate atherosclerosis in HFD-fed apoE-/- mice, as evidenced by the increase in plaque size and volume in the aortic walls observed via Oil Red O staining. 16S rRNA sequencing revealed significant alterations in the gut microbiota, with harmful bacterial species thriving while beneficial species declining. Metabolomic profiling indicated disruptions in lipid metabolism and primary bile acid synthesis, leading to elevated levels of taurochenodeoxycholic acid (TCDCA), taurocholic acid (TCA), and tauroursodeoxycholic acid (TDCA). These metabolic shifts may contribute to atherosclerosis development. Furthermore, impaired intestinal barrier function, characterized by reduced mucin expression and disrupted tight junction proteins, was observed. The increased intestinal permeability observed was positively correlated with the severity of atherosclerotic lesions, highlighting the importance of the intestinal barrier in cardiovascular health. In conclusion, this research underscores the intricate interplay among oral health, gut microbiota composition, metabolite profiles, and CVD incidence. These findings emphasize the importance of maintaining good oral hygiene as a potential preventive measure against cardiovascular issues, as well as the need for further investigations into the intricate mechanisms linking oral health, gut microbiota, and metabolic pathways in CVD development.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
