

Association between pretreatment emotional distress and immune checkpoint inhibitor response in non-small-cell lung cancer
- PMID: 38740994
- PMCID: PMC11186781
- DOI: 10.1038/s41591-024-02929-4
Association between pretreatment emotional distress and immune checkpoint inhibitor response in non-small-cell lung cancer
Abstract
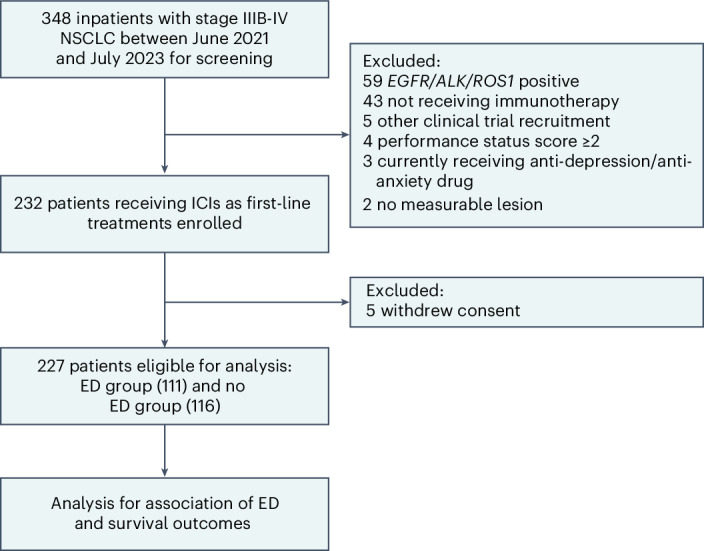
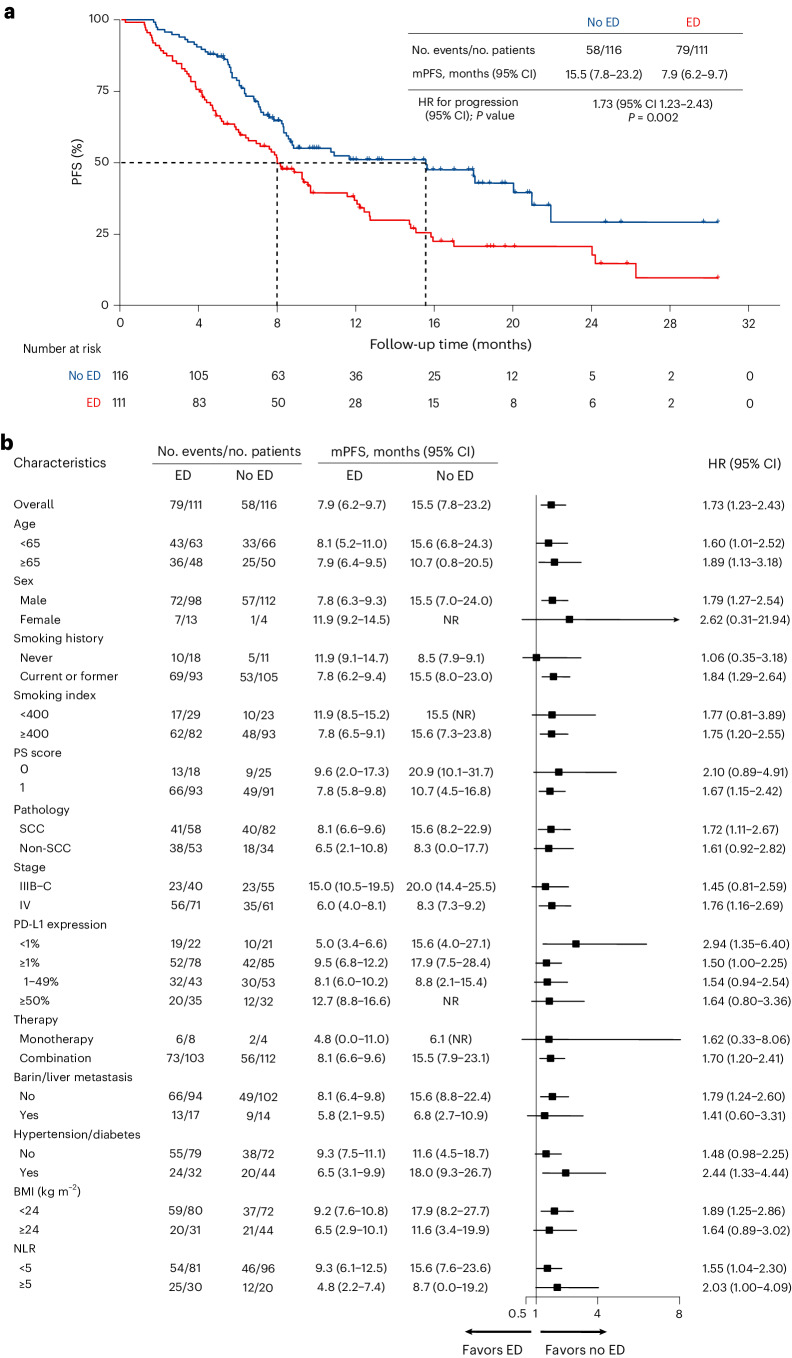
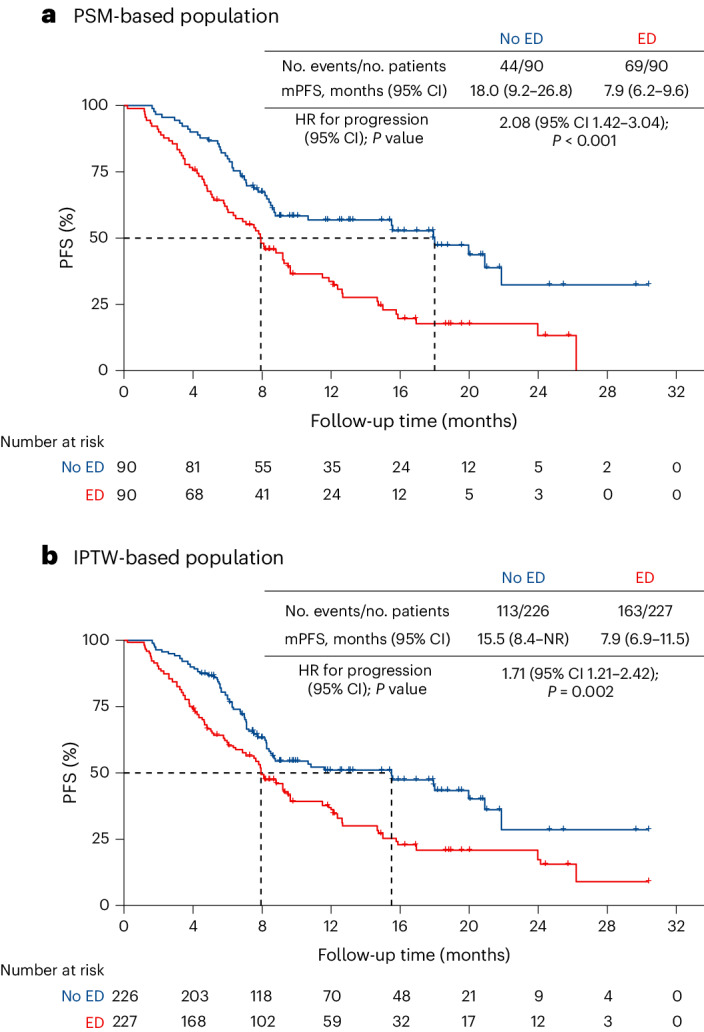
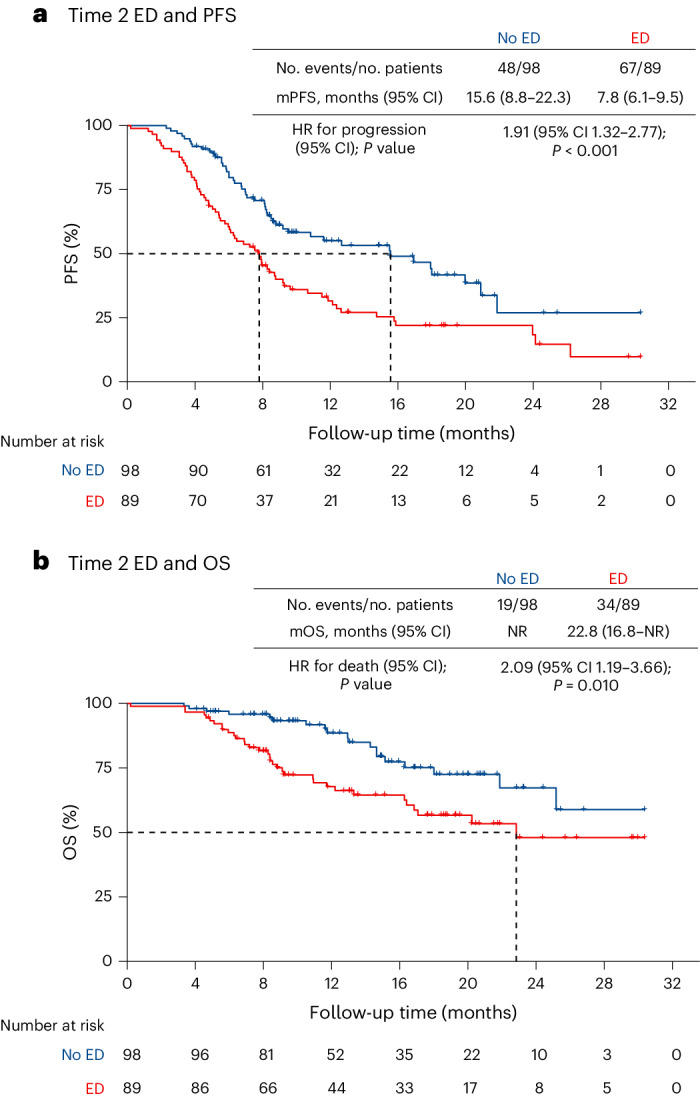
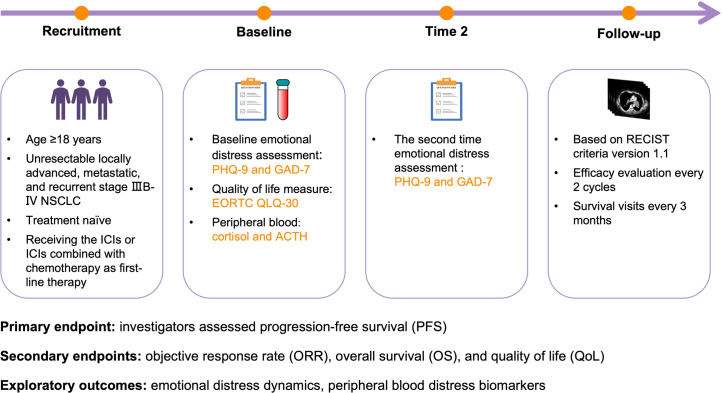
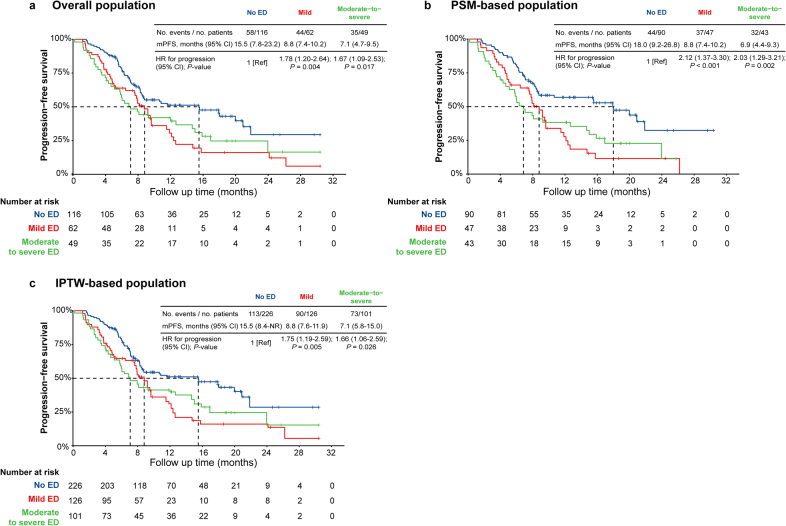
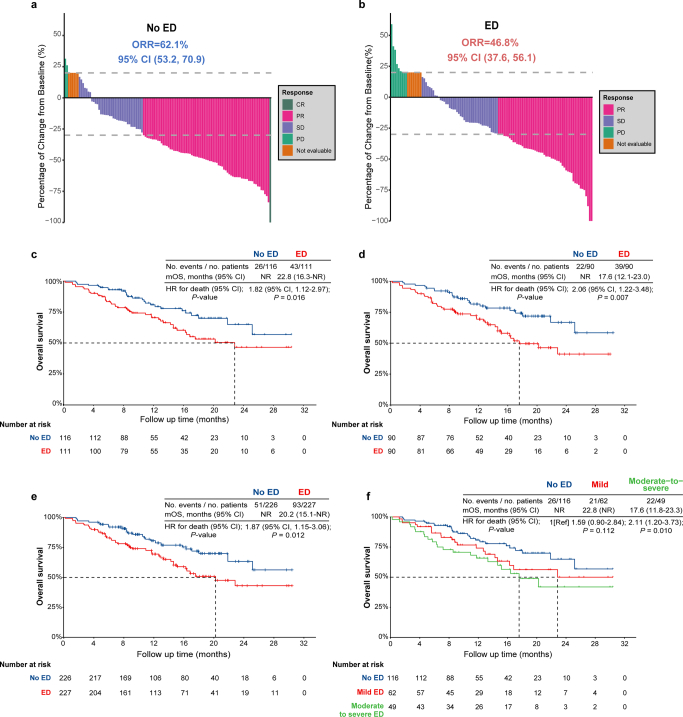
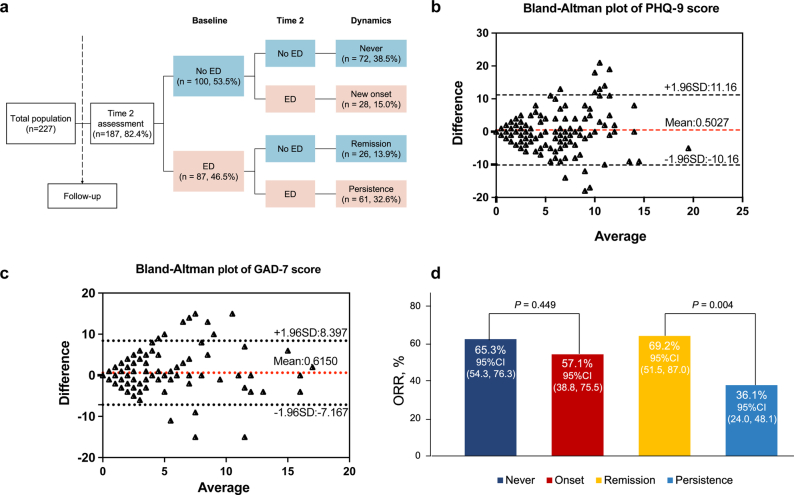
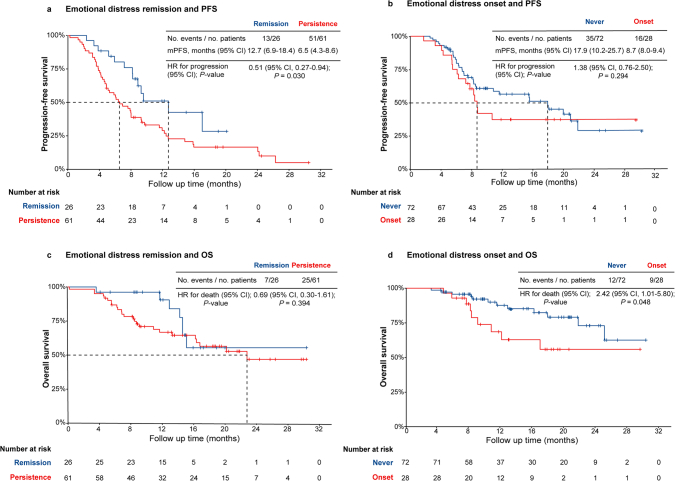
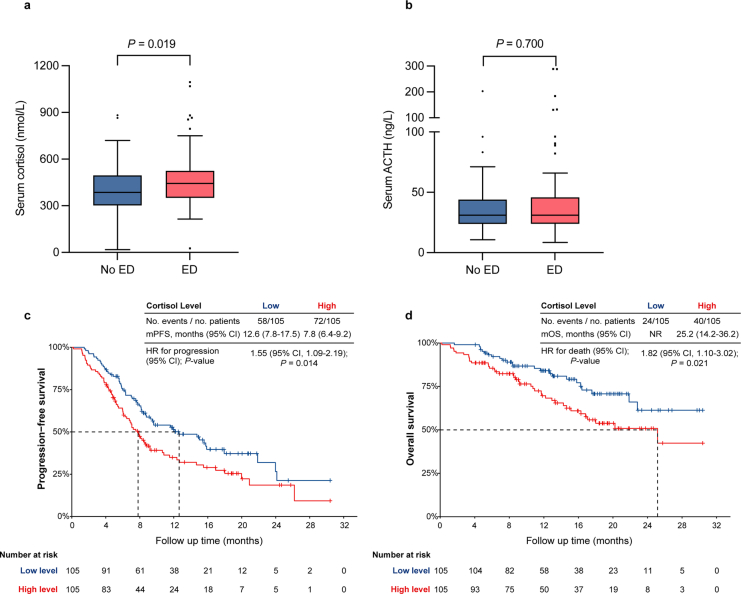
Emotional distress (ED), commonly characterized by symptoms of depression and/or anxiety, is prevalent in patients with cancer. Preclinical studies suggest that ED can impair antitumor immune responses, but few clinical studies have explored its relationship with response to immune checkpoint inhibitors (ICIs). Here we report results from cohort 1 of the prospective observational STRESS-LUNG study, which investigated the association between ED and clinical efficacy of first-line treatment of ICIs in patients with advanced non-small-cell lung cancer. ED was assessed by Patient Health Questionnaire-9 and Generalized Anxiety Disorder 7-item scale. The study included 227 patients with 111 (48.9%) exhibiting ED who presented depression (Patient Health Questionnaire-9 score ≥5) and/or anxiety (Generalized Anxiety Disorder 7-item score ≥5) symptoms at baseline. On the primary endpoint analysis, patients with baseline ED exhibited a significantly shorter median progression-free survival compared with those without ED (7.9 months versus 15.5 months, hazard ratio 1.73, 95% confidence interval 1.23 to 2.43, P = 0.002). On the secondary endpoint analysis, ED was associated with lower objective response rate (46.8% versus 62.1%, odds ratio 0.54, P = 0.022), reduced 2-year overall survival rate of 46.5% versus 64.9% (hazard ratio for death 1.82, 95% confidence interval 1.12 to 2.97, P = 0.016) and detriments in quality of life. The exploratory analysis indicated that the ED group showed elevated blood cortisol levels, which was associated with adverse survival outcomes. This study suggests that there is an association between ED and worse clinical outcomes in patients with advanced non-small-cell lung cancer treated with ICIs, highlighting the potential significance of addressing ED in cancer management. ClinicalTrials.gov registration: NCT05477979 .
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Patient-focused insights: how emotional distress shapes immunotherapy response in non-small cell lung cancer.Transl Lung Cancer Res. 2024 Dec 31;13(12):3819-3823. doi: 10.21037/tlcr-24-904. Epub 2024 Dec 27. Transl Lung Cancer Res. 2024. PMID: 39830766 Free PMC article. No abstract available.
-
Emotional distress: the hidden barrier to immunotherapy success in advanced non-small cell lung cancer.Transl Lung Cancer Res. 2025 May 30;14(5):1877-1881. doi: 10.21037/tlcr-2025-31. Epub 2025 May 14. Transl Lung Cancer Res. 2025. PMID: 40535064 Free PMC article. No abstract available.
References
-
- Passaro A, Brahmer J, Antonia S, Mok T, Peters S. Managing resistance to immune checkpoint inhibitors in lung cancer: treatment and novel strategies. J. Clin. Oncol. 2022;40:598–610. - PubMed
-
- Mino-Kenudson M, et al. Predictive biomarkers for immunotherapy in lung cancer: perspective from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2022;17:1335–1354. - PubMed
-
- Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. Br. Med. J. 2018;361:k1415. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- kq1907077/Science and Technology Bureau, Changsha (Changsha Municipal Science and Technology Bureau)
- 295228/Education Department of Hunan Province (Hunan Province Education Department)
- Y-HS202102-0130/Chinese Society of Clinical Oncology (Chinese Society of Clinical Oncology, Beijing Xisike Clinical Oncology Research Foundation)
- 82272806/National Natural Science Foundation of China (National Science Foundation of China)
- 2021JJ20088/Natural Science Foundation of Hunan Province (Hunan Provincial Natural Science Foundation)
LinkOut - more resources
Full Text Sources
Medical
