

An epidemiological and clinicopathological study of type 1 vs. type 2 morphological subtypes of papillary renal cell carcinoma- results from a nation-wide study covering 50 years in Iceland
- PMID: 38741053
- PMCID: PMC11089793
- DOI: 10.1186/s12894-024-01494-9
An epidemiological and clinicopathological study of type 1 vs. type 2 morphological subtypes of papillary renal cell carcinoma- results from a nation-wide study covering 50 years in Iceland
Abstract
Introduction: Papillary renal cell carcinoma (pRCC) is the second most common histology of renal cell carcinoma (RCC), accounting for 10-15% of cases. Traditionally, pRCC is divided into type 1 and type 2, although this division is currently debated as a prognostic factor of survival. Our aim was to investigate the epidemiology and survival of the pRCC subtypes in a whole nation cohort of patients during a 50-year period.
Materials and methods: A Population based retrospective study including consecutive cases of RCC in Iceland from 1971-2020. Comparisons were made between histological classifications of RCC, with emphasis on pRCC subtypes (type 1 vs. 2) for outcome estimation. Changes in RCC incidence were analyzed in 5-year intervals after age standardization. The Kaplan-Meier method and Cox regression were used for outcome analysis.
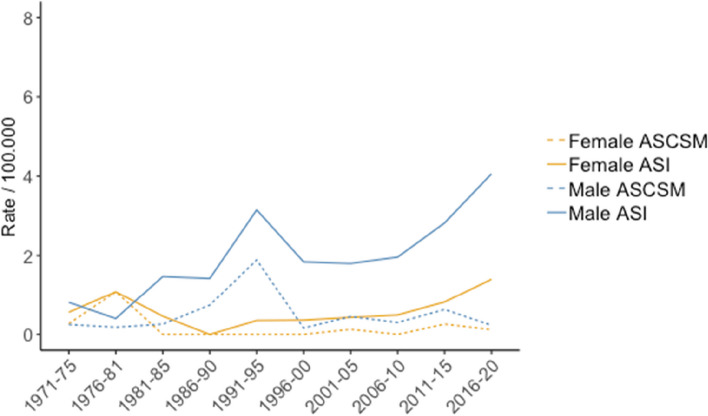
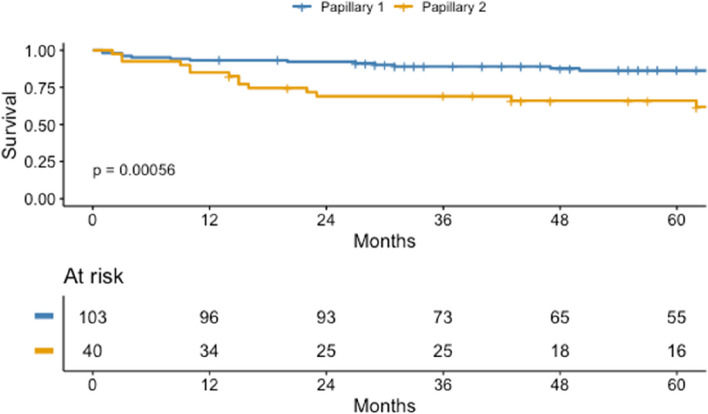
Results: A total of 1.725 cases were identified, with 74.4%, 2.1% and 9.2% having clear cell (ccRCC), chromophobe (chRCC), and pRCC, respectively. The age standardized incidence (ASI) of pRCC was 1.97/100.000 for males and 0.5/100.000 for females, and the proportion of pRCC increased from 3.7% to 11.5% between the first and last intervals of the study (p < 0.001). Age standardized cancer specific mortality (ASCSM) of pRCC was 0.6/100.000 and 0.19/100.000 for males and females, respectively. The annual average increase in ASI was 3.6% for type 1 pRCC, but the ASI for type 2 pRCC and ASCSM for both subtypes did not change significantly. Male to female ratio was 4.4 for type 1 pRCC and 2.3 for type 2. The average tumor size for type 1 and 2 was 58.8 and 73.7 mm, respectively. Metastasis at diagnosis was found in 8.7% in the type 1 pRCC, compared to 30.0% of patients with type 2 pRCC (p < 0.001). Estimated 5-year cancer-specific survival (CSS) were 94.4%, 80.7%, and 69.3% for chRCC, pRCC and ccRCC, respectively (p < 0.001). For the pRCC subtypes, type 1 was associated with better 5-year CSS than type 2 (86.3% vs. 66.0%, p < 0.001), although this difference was not significant after adjusting for cancer stage and grading.
Conclusions: pRCC histology was slightly less common in Iceland than in other countries. Males are more than three times more likely to be diagnosed with pRCC, compared to other RCC histologies. The subtype of pRCC was not found to be an independent risk factor for worse survival, and as suggested by the most recent WHO Classification of Urinary Tumors, grade and TNM-stage seem to be the most important factors for estimation of survival for pRCC patients.
Keywords: Histology; Incidence; Kidney cancer; Mortality; Papillary renal cell carcinoma; Prognosis; Renal cancer; Renal cell carcinoma; Subtyping; Survival.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Delahunt B, Eble JN. Papillary renal cell carcinoma: a clinicopathologic and immunohistochemical study of 105 tumors. Mod Pathol. 1997;10(6):537–544. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
