

Incidences of colorectal adenomas and cancers under colonoscopy surveillance suggest an accelerated "Big Bang" pathway to CRC in three of the four Lynch syndromes
- PMID: 38741120
- PMCID: PMC11089795
- DOI: 10.1186/s13053-024-00279-3
Incidences of colorectal adenomas and cancers under colonoscopy surveillance suggest an accelerated "Big Bang" pathway to CRC in three of the four Lynch syndromes
Abstract
Background: Colorectal cancers (CRCs) in the Lynch syndromes have been assumed to emerge through an accelerated adenoma-carcinoma pathway. In this model adenomas with deficient mismatch repair have an increased probability of acquiring additional cancer driver mutation(s) resulting in more rapid progression to malignancy. If this model was accurate, the success of colonoscopy in preventing CRC would be a function of the intervals between colonoscopies and mean sojourn time of detectable adenomas. Contrary to expectations, colonoscopy did not decrease incidence of CRC in the Lynch syndromes and shorter colonoscopy intervals have not been effective in reducing CRC incidence. The prospective Lynch Syndrome Database (PLSD) was designed to examine these issues in carriers of pathogenic variants of the mis-match repair (path_MMR) genes.
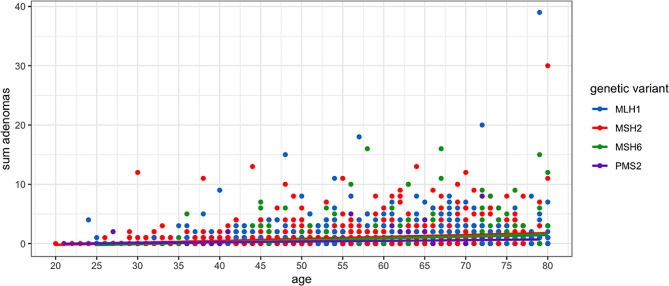
Materials and methods: We examined the CRC and colorectal adenoma incidences in 3,574 path_MLH1, path_MSH2, path_MSH6 and path_PMS2 carriers subjected to regular colonoscopy with polypectomy, and considered the results based on sojourn times and stochastic probability paradigms.
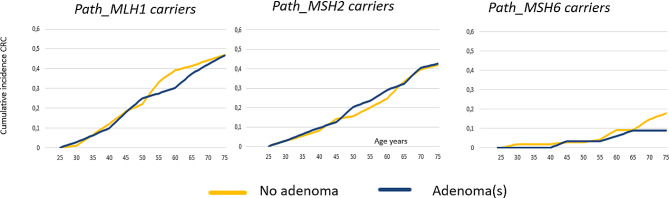
Results: Most of the path_MMR carriers in each genetic group had no adenomas. There was no association between incidences of CRC and the presence of adenomas. There was no CRC observed in path_PMS2 carriers.
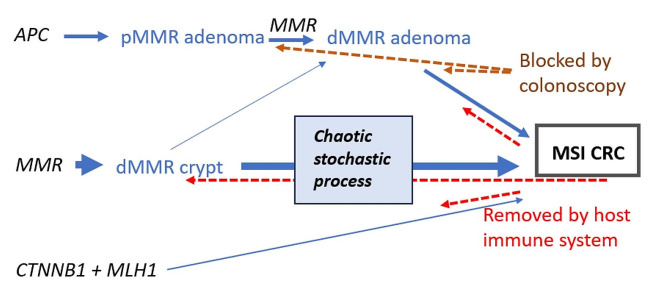
Conclusions: Colonoscopy prevented CRC in path_PMS2 carriers but not in the others. Our findings are consistent with colonoscopy surveillance blocking the adenoma-carcinoma pathway by removing identified adenomas which might otherwise become CRCs. However, in the other carriers most CRCs likely arised from dMMR cells in the crypts that have an increased mutation rate with increased stochastic chaotic probabilities for mutations. Therefore, this mechanism, that may be associated with no or only a short sojourn time of MSI tumours as adenomas, could explain the findings in our previous and current reports.
Keywords: MLH1; MSH2; MSH6; PMS2; Adenoma; Colonoscopy; Colorectal; Lynch syndromes; MSI; Sojourn time; cancer; dMMR.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- https://www.omim.org/ Accessed April 2nd 2024.
Grants and funding
- Contract 194751-2017/The Norwegian Cancer Society
- Contract 194751-2017/The Norwegian Cancer Society
- Contract 194751-2017/The Norwegian Cancer Society
- IS-BRC-1215-20007/Manchester National Institute for Health Research (NIHR) Biomedical Research Centre
- IS-BRC-1215-20007/Manchester National Institute for Health Research (NIHR) Biomedical Research Centre
LinkOut - more resources
Full Text Sources
Miscellaneous
