

HMGB1 Expression Levels Correlate with Response to Immunotherapy in Non-Small Cell Lung Cancer
- PMID: 38741920
- PMCID: PMC11090191
- DOI: 10.2147/LCTT.S455034
HMGB1 Expression Levels Correlate with Response to Immunotherapy in Non-Small Cell Lung Cancer
Abstract
Purpose: High-mobility group box 1 protein (HMGB1) is subject to exportin 1 (XPO1)-dependent nuclear export, and it is involved in functions implicated in resistance to immunotherapy. We investigated whether HMGB1 mRNA expression was associated with response to immune checkpoint inhibitors (ICI) in non-small cell lung cancer (NSCLC).
Patients and methods: RNA was isolated from pretreatment biopsies of patients with advanced NSCLC treated with ICI. Gene expression analysis of several genes, including HMGB1, was conducted using the NanoString Counter analysis system (PanCancer Immune Profiling Panel). Western blotting analysis and cell viability assays in EGFR and KRAS mutant cell lines were carried out. Evaluation of the antitumoral effect of ICI in combination with XPO1 blocker (selinexor) and trametinib was determined in a murine Lewis lung carcinoma model.
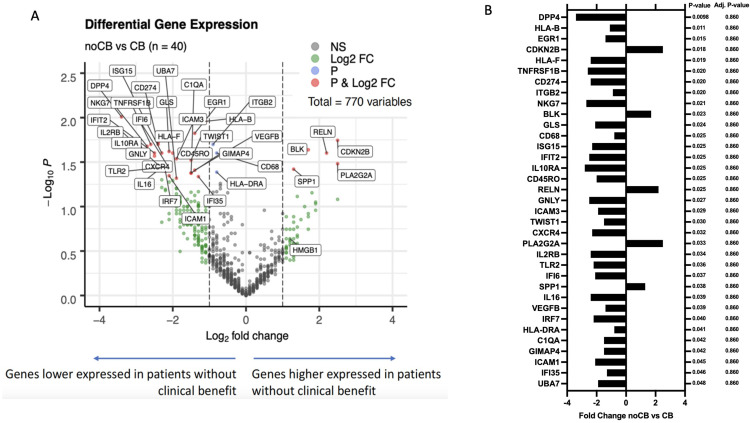
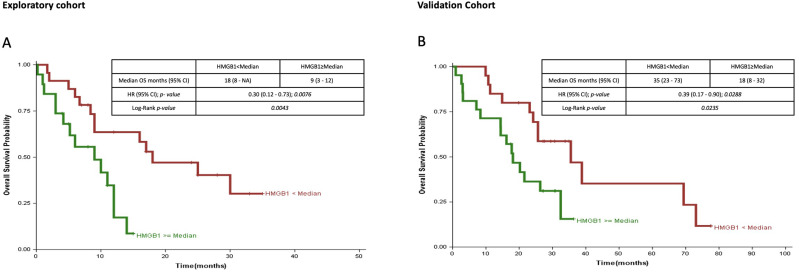
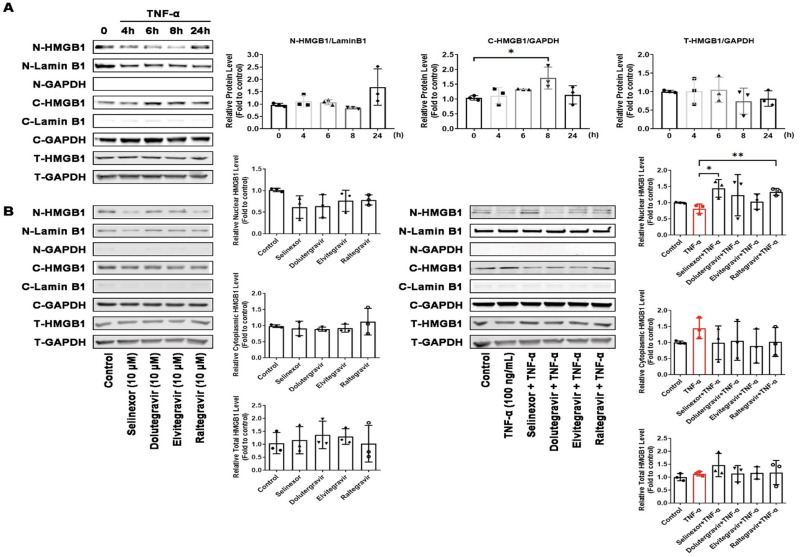
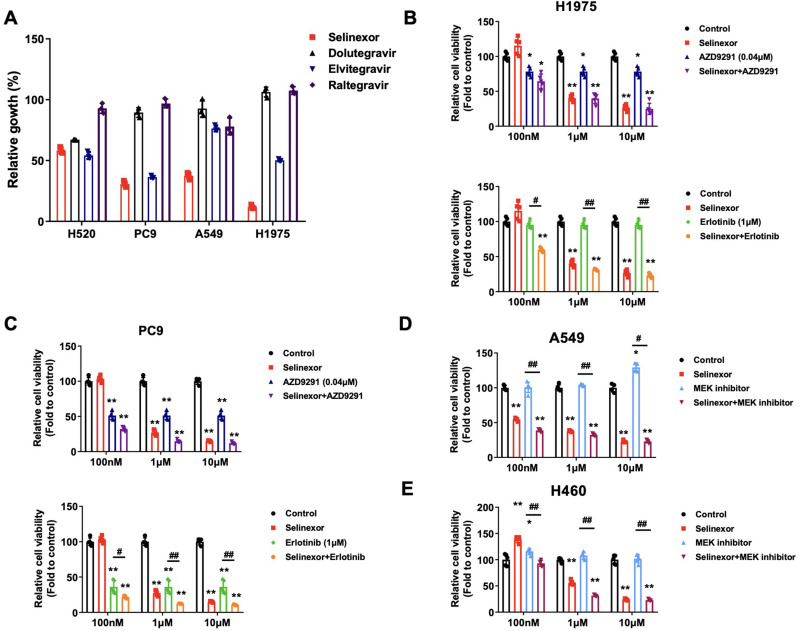
Results: HMGB1 mRNA levels in NSCLC patients treated with ICI correlated with progression-free survival (PFS) (median PFS 9.0 versus 18.0 months, P=0.008, hazard ratio=0.30 in high versus low HMGB1). After TNF-α stimulation, HMGB1 accumulates in the cytoplasm of PC9 cells, but this accumulation can be prevented by using selinexor or antiretroviral drugs. Erlotinib or osimertinib with selinexor in EGFR-mutant cells and trametinib plus selinexor in KRAS mutant abolish tumor cell proliferation. Selinexor with a PD-1 inhibitor with or without trametinib abrogates the tumor growth in the murine Lewis lung cancer model.
Conclusion: An in-depth exploration of the functions of HMGB1 mRNA and protein is expected to uncover new potential targets and provide a basis for treating metastatic NSCLC in combination with ICI.
Keywords: HMGB1; K-Ras mutations; Lewis lung cancer murine model; immunotherapy; non-small cell lung cancer.
© 2024 González-Cao et al.
Conflict of interest statement
Dr Andrés Aguilar reports personal fee and/or non-financial support for congress, travel and/or speaker honoraria from MERCK SHARP and DOHME, Janssen-Cilag S.A., ROCHE-FARMA SA, TAKEDA ONCOLOGY, Bristol-Myers Squibb, outside the submitted work. The authors declare that they have no other known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
