

Minimally Invasive Approaches in the Surgical Treatment of Intracranial Meningiomas: An Analysis of 54 Cases
- PMID: 38742257
- PMCID: PMC11096627
- DOI: 10.14791/btrt.2024.0005
Minimally Invasive Approaches in the Surgical Treatment of Intracranial Meningiomas: An Analysis of 54 Cases
Abstract
Background: Intracranial meningiomas, being a fairly common disease in the population, often require surgical treatment, which, in turn, can completely heal the patient. The localization of meningiomas often influences treatment even if they are asymptomatic. By modernizing approaches to surgical treatment, it is possible to minimize intra- and postoperative risks, while achieving complete removal of the tumor. One of these methods is minimally invasive neurosurgery, the development of which in recent years allows it to compete with standard surgical methods. The purpose of this study was the objectification of minimally invasive approaches, such as the calculation of the craniotomy area and the ratio of craniotomy area to the resected tumor volume.
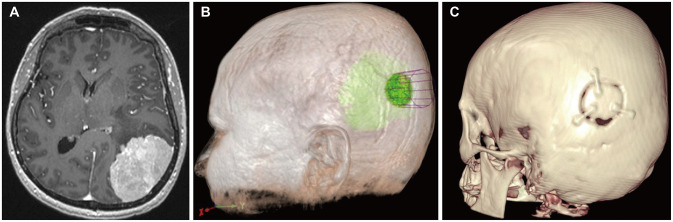
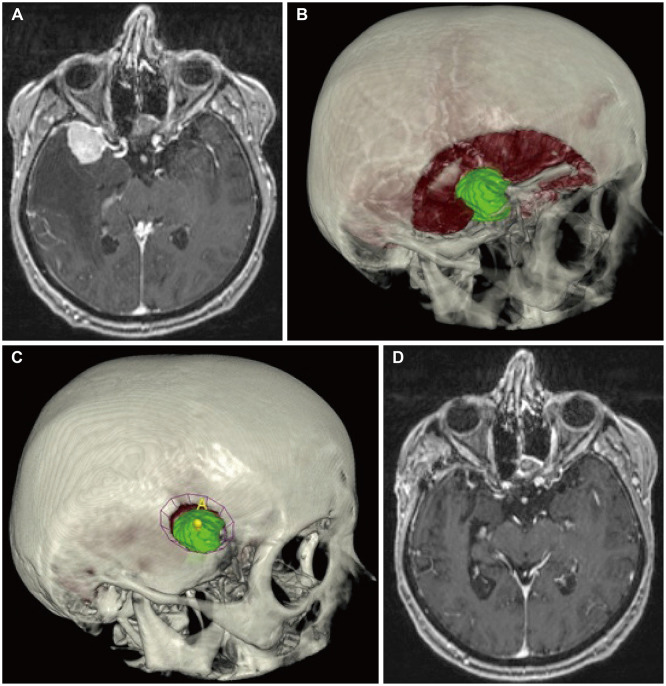
Methods: The retrospective study consisted of a group of 54 consecutive patients who were operated on in our neurosurgery clinic specialized on minimally invasive neurosurgery. Preoperative planning was carried out using the Surgical Theater visualization platform. Using this system, the tumor volume and craniotomy surface area were calculated. During the analysis, the symptoms before and after the surgery, classification of tumors, postoperative complications, further treatment and follow-up results were assessed.
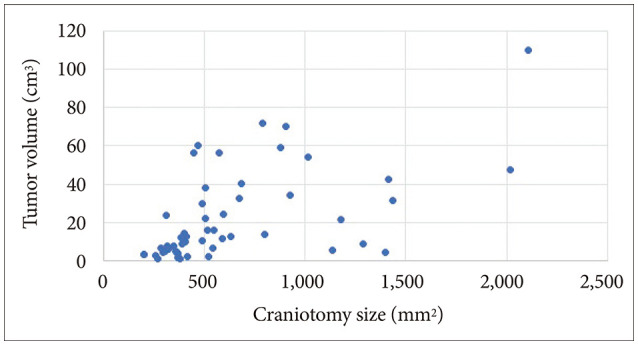
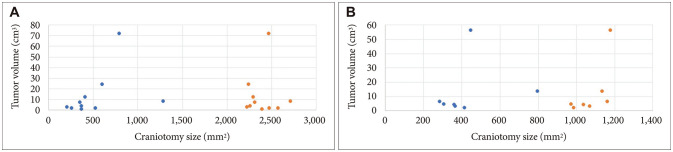
Results: Twelve (22.2%) patients were men and 42 (77.8%) were women. The mean age of the group was 64.2 years (median 67.5). The craniotomy area ranged from 202 to 2,108 mm² (mean 631 mm²). Tumor volume ranged from 0.85 to 110.1 cm3 (mean 21.6 cm3). The craniotomy size of minimally invasive approaches to the skull base was 3-5 times smaller than standard approaches. Skull base meningiomas accounted for 19 cases (35.2%), convexity meningiomas for 26 cases (48.1%), and falx and tentorium meningiomas for 9 cases (16.7%). Three complications were reported: postoperative hemorrhage, CSF leakage, and ophthalmoplegia. Relapse was detected in 2 patients with a mean follow-up of 26.3 months (median 20).
Conclusion: Minimally invasive approaches in the surgical treatment of intracranial meningiomas reduce the possibility of operating trauma by several times; they are safe and sufficient for complete removal of the tumor.
Keywords: Intracranial meningioma; Minimally invasive approach; Skull base.
Copyright © 2024 The Korean Brain Tumor Society, The Korean Society for Neuro-Oncology, and The Korean Society for Pediatric Neuro-Oncology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Staneczek W, Jänisch W. Epidemiologic data on meningiomas in East Germany 1961-1986: incidence, localization, age and sex distribution. Clin Neuropathol. 1992;11:135–141. - PubMed
-
- Codd MB, Kurland LT. Descriptive epidemiology of primary intracranial neoplasms. Prog Exp Tumor Res. 1985;29:1–11. - PubMed
