

Influence of Pathophysiologic Patterns of Coronary Artery Disease on Immediate Percutaneous Coronary Intervention Outcomes
- PMID: 38742491
- PMCID: PMC11335079
- DOI: 10.1161/CIRCULATIONAHA.124.069450
Influence of Pathophysiologic Patterns of Coronary Artery Disease on Immediate Percutaneous Coronary Intervention Outcomes
Abstract
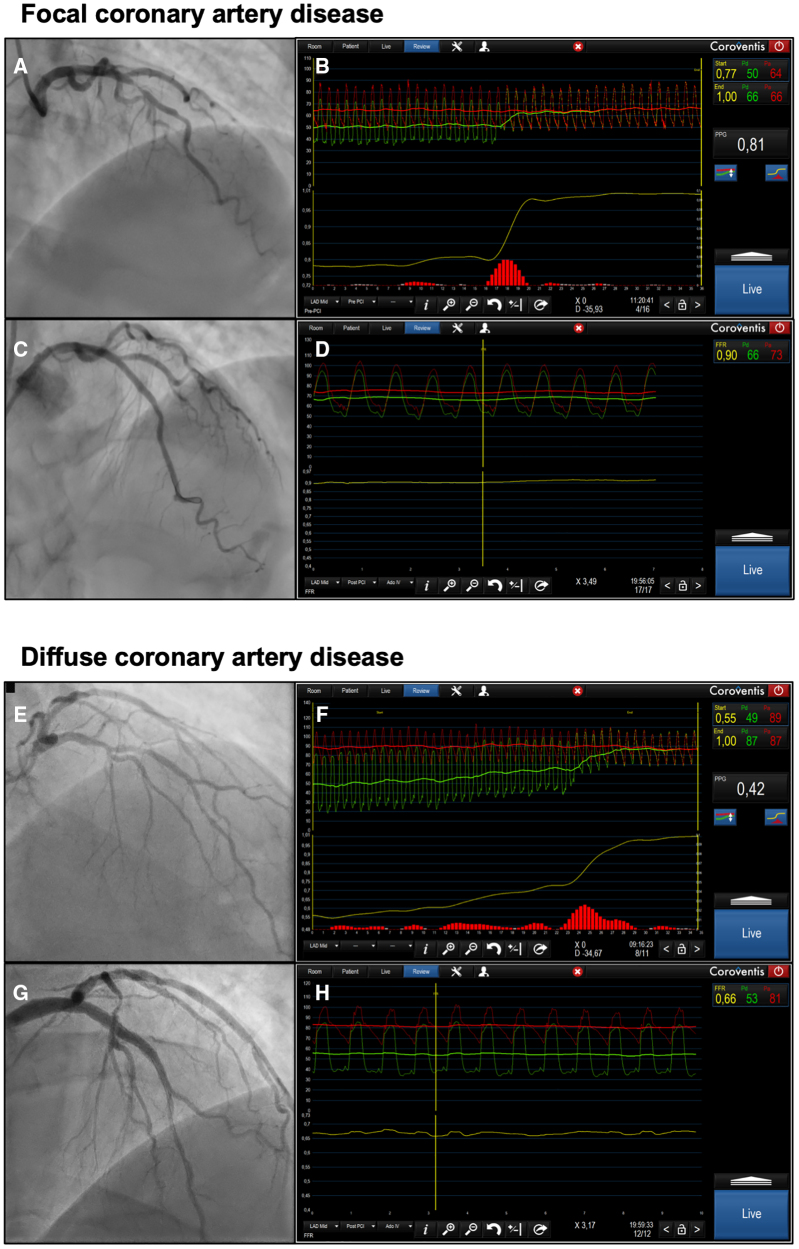
Background: Diffuse coronary artery disease affects the safety and efficacy of percutaneous coronary intervention (PCI). Pathophysiologic coronary artery disease patterns can be quantified using fractional flow reserve (FFR) pullbacks incorporating the pullback pressure gradient (PPG) calculation. This study aimed to establish the capacity of PPG to predict optimal revascularization and procedural outcomes.
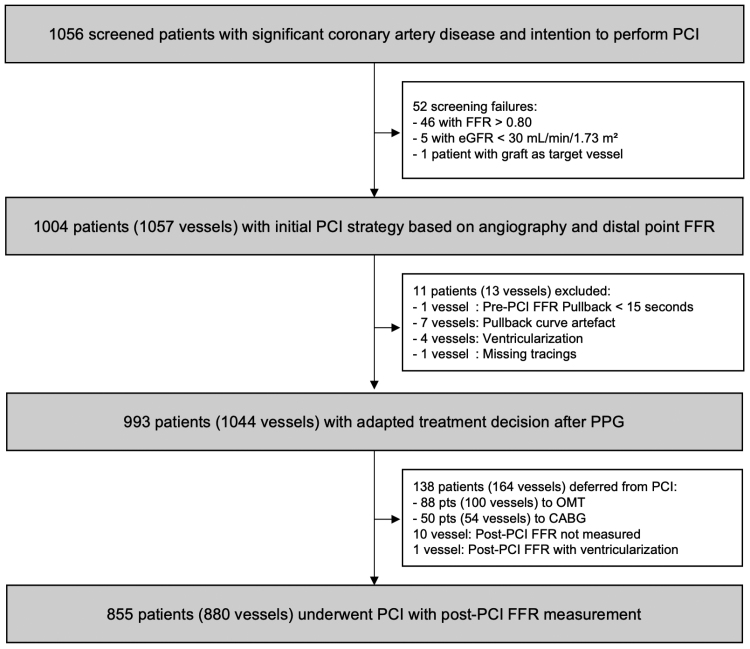
Methods: This prospective, investigator-initiated, single-arm, multicenter study enrolled patients with at least one epicardial lesion with an FFR ≤0.80 scheduled for PCI. Manual FFR pullbacks were used to calculate PPG. The primary outcome of optimal revascularization was defined as an FFR ≥0.88 after PCI.
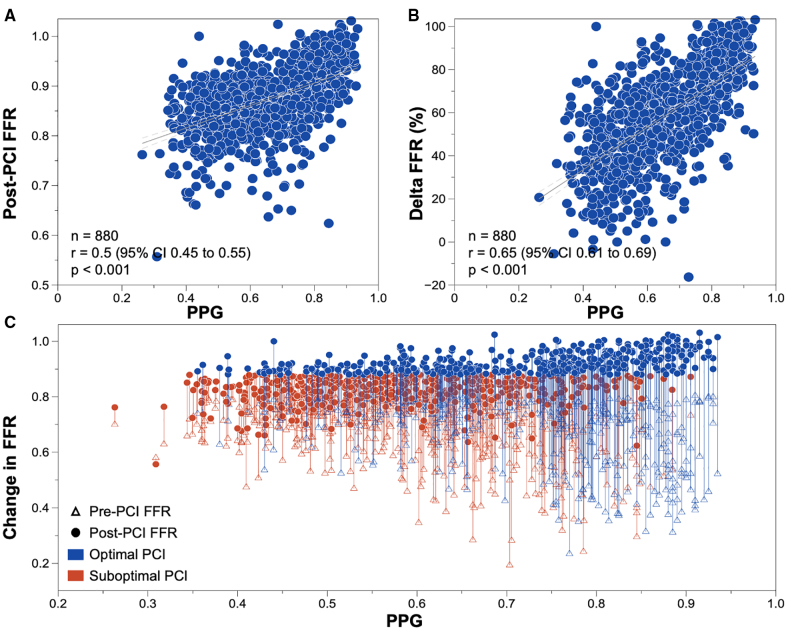
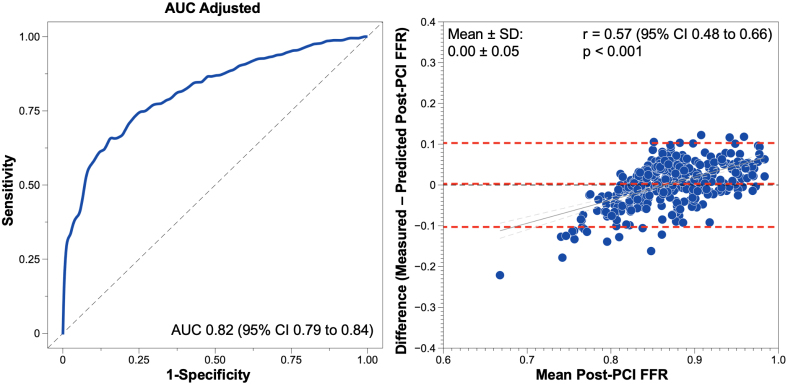
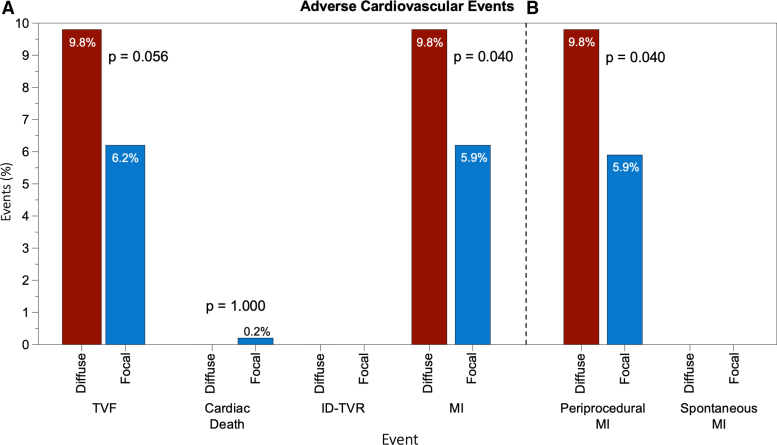
Results: A total of 993 patients with 1044 vessels were included. The mean FFR was 0.68±0.12, PPG 0.62±0.17, and the post-PCI FFR was 0.87±0.07. PPG was significantly correlated with the change in FFR after PCI (r=0.65 [95% CI, 0.61-0.69]; P<0.001) and demonstrated excellent predictive capacity for optimal revascularization (area under the receiver operating characteristic curve, 0.82 [95% CI, 0.79-0.84]; P<0.001). FFR alone did not predict revascularization outcomes (area under the receiver operating characteristic curve, 0.54 [95% CI, 0.50-0.57]). PPG influenced treatment decisions in 14% of patients, redirecting them from PCI to alternative treatment modalities. Periprocedural myocardial infarction occurred more frequently in patients with low PPG (<0.62) compared with those with focal disease (odds ratio, 1.71 [95% CI, 1.00-2.97]).
Conclusions: Pathophysiologic coronary artery disease patterns distinctly affect the safety and effectiveness of PCI. PPG showed an excellent predictive capacity for optimal revascularization and demonstrated added value compared with an FFR measurement.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT04789317.
Keywords: coronary artery disease; hemodynamics; percutaneous coronary intervention.
Conflict of interest statement
Dr Collet reports receiving research grants from Biosensors, Coroventis Research, Medis Medical Imaging, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott Vascular; consultancy fees from HeartFlow, OpSens Medical, Abbott Vascular, and Philips Volcano; and has patents pending on diagnostic methods for coronary artery disease. Dr Munhoz reports a research grant provided by the CardioPath PhD programme and speaker fees from Abbott Vascular. Dr Mizukami reports receiving research grants from Boston Scientific and speaker fees from Abbott Vascular, CathWorks, and Boston Scientific. Dr Matsuo has received consulting fees from Kaneka and Zeon and speaker’s fees from Abbott Medical Japan, Boston Scientific, Philips, and Amgen. Dr Ko has received consulting fees from Canon Medical, Abbott, and Medtronic. Dr Biscaglia received research grants provided by Sahajanand Medical Technologies, Medis Medical Imaging, Eukon Srl, Siemens Healthineers, General Electric Healthcare, and Insight Lifetech. Dr Engstrøm reports speaker and advisory board fees from Abbott, Boston Scientific, and Novo Nordisk. Dr Leone reports receiving consultancy fees from Abbott and honoraria for sponsored symposia from Abbott, Medtronic, and Abiomed. Dr Fearon receives institutional research support from Abbott, Boston Scientific, and Medtronic and has consulting relationships with CathWorks and Siemens and stock options from HeartFlow. Dr Christiansen has received consulting fees from Abbott Medical Denmark A/S. Dr Yong has received minor honoraria from Abbott Vascular and research grants from Abbott Vascular and Philips. Dr Escaned is supported by the Intensification of Research Activity project INT22/00088 from the Spanish Instituto de Salud Carlos III and received speaker and advisory board member fees from Abbott and Philips. Dr Storozhenko reports a grant provided by the EAPCI Fellowship Programme. Dr West is an employee of Abbott Vascular. Dr De Potter is a paid consultant for Biosense Webster and receives grant support (institutional) and consultancy fees (institutional) from Abbott. Dr Berry receives research funding from the British Heart Foundation (grants RE/18/6134217, BHF/FS/17/26/32744, and PG/19/28/34310) and is employed by the University of Glasgow, which holds consultancy and research agreements for his work with Abbott Vascular, AstraZeneca, Boehringer Ingelheim, Coroventis Research, GlaxoSmithKline, HeartFlow, Menarini, Novartis, Servier, Siemens Healthcare, and Valo Health. Dr Collison has received consulting fees from Abbott. Dr Johnson has received consultancy or speaker fees from Abbott Vascular, Boston Scientific, Medtronic, Shockwave, and Terumo, and research grants from Abbott Vascular. Dr Amano reports receiving lecture fees from Astellas Pharma, Astra Zeneca, Bayer, Daiichi Sankyo, and Bristol Myers Squibb. Dr Perera has received research grant support from Abbott Vascular, HeartFlow, and Philips. Dr Jeremias has received consulting fees from Canon Medical, Artrya Medical, and Boston Scientific. Dr Ali reports institutional grant support from Abbott, Abiomed, Acist, Amgen, Boston Scientific, CathWorks, Canon Medical, Conavi, HeartFlow, Inari, Medtronic, the US National Institutes of Health, Nipro, OpSens Medical, Medis, Philips, Shockwave, Siemens, SpectraWAVE, and Teleflex; consulting fees from Abiomed, Astra Zeneca, Boston Scientific, CathWorks, OpSens Medical, Philips, and Shockwave; and equity in Elucid, Lifelink, SpectraWAVE, Shockwave, and VitalConnect. Dr Pijls has received research grants from Abbott and Hexacath; consultancy fees from Abbott, GE, Philips, and HeartFlow; and has equity in General Electric, Philips, and HeartFlow. Dr De Bruyne reports receiving consultancy fees from Boston Scientific and Abbott and research grants from Coroventis Research, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott Vascular. Dr Johnson received internal funding from the Weatherhead PET Center for Preventing and Reversing Atherosclerosis; has received significant institutional research support from St Jude Medical (CONTRAST [Can Contrast Injection Better Approximate FFR Compared to Pure Resting Physiology?; URL: https://www.clinicaltrials.gov; Unique identifier: NCT02184117]) and Philips Volcano (DEFINE-FLOW [Combined Pressure and Flow Measurements to Guide Treatment of Coronary Stenoses; URL: https://www.clinicaltrials.gov; Unique identifier: NCT02328820]) for other studies using intracoronary pressure and flow sensors; has an institutional licensing agreement with Boston Scientific for the smart-minimum FFR algorithm (now commercialized under 510[k] K191008); and has patents pending on diagnostic methods for quantifying aortic stenosis and TAVI physiology and on methods to correct pressure tracings from fluid-filled catheters.
Figures
Comment in
-
Does PPG, the Other Dimension to FFR, Better Predict Post-PCI Results?Circulation. 2024 Aug 20;150(8):598-599. doi: 10.1161/CIRCULATIONAHA.124.070439. Epub 2024 Aug 19. Circulation. 2024. PMID: 39159226 No abstract available.
References
-
- Collison D, Copt S, Mizukami T, Collet C, McLaren R, Didagelos M, Aetesam-Ur-Rahman M, McCartney P, Ford TJ, Lindsay M, et al. . Angina after percutaneous coronary intervention: patient and procedural predictors. Circ Cardiovasc Interv. 2023;16:e012511. doi: 10.1161/CIRCINTERVENTIONS.122.012511 - PMC - PubMed
-
- Collet C, Sonck J, Vandeloo B, Mizukami T, Roosens B, Lochy S, Argacha J-F, Schoors D, Colaiori I, Di Gioia G, et al. . Measurement of hyperemic pullback pressure gradients to characterize patterns of coronary atherosclerosis. J Am Coll Cardiol. 2019;74:1772–1784. doi: 10.1016/j.jacc.2019.07.072 - PubMed
-
- Collet C, Collison D, Mizukami T, McCartney P, Sonck J, Ford T, Munhoz D, Berry C, De Bruyne B, Oldroyd K. Differential improvement in angina and health-related quality of life after PCI in focal and diffuse coronary artery disease. JACC Cardiovasc Interv. 2022;15:2506–2518. doi: 10.1016/j.jcin.2022.09.048 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
