

Perivascular NOTCH3+ Stem Cells Drive Meningioma Tumorigenesis and Resistance to Radiotherapy
- PMID: 38742767
- PMCID: PMC11452293
- DOI: 10.1158/2159-8290.CD-23-1459
Perivascular NOTCH3+ Stem Cells Drive Meningioma Tumorigenesis and Resistance to Radiotherapy
Abstract
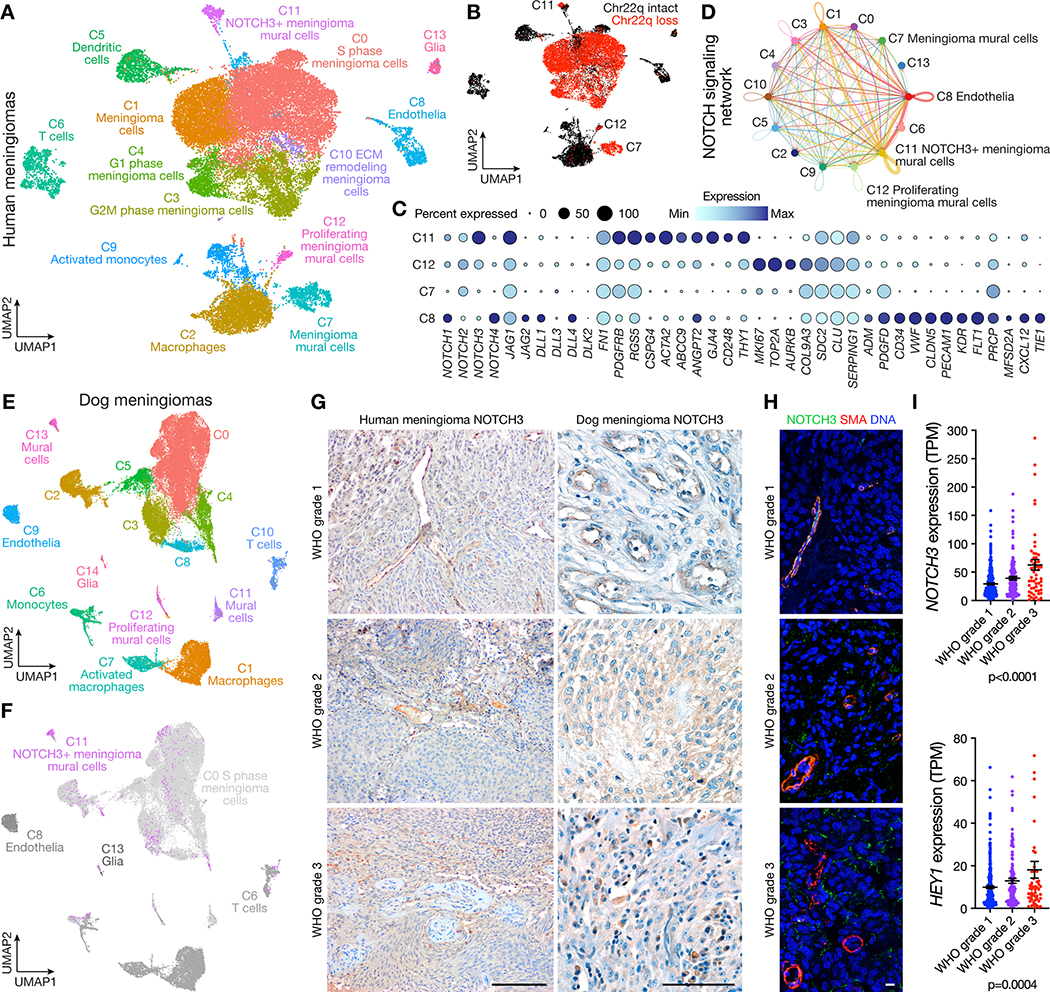
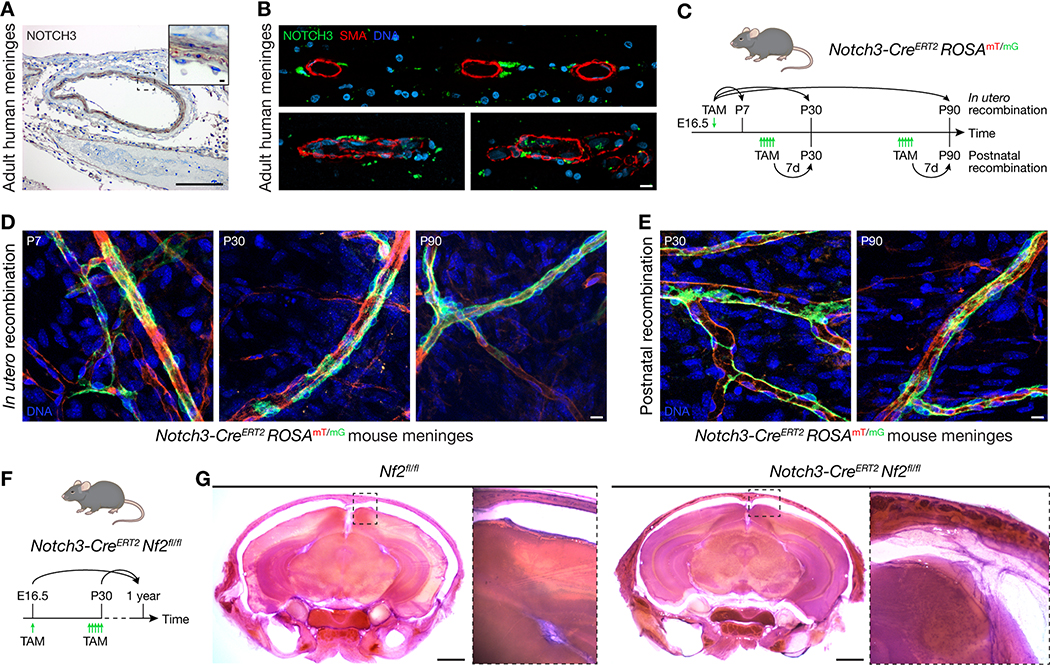
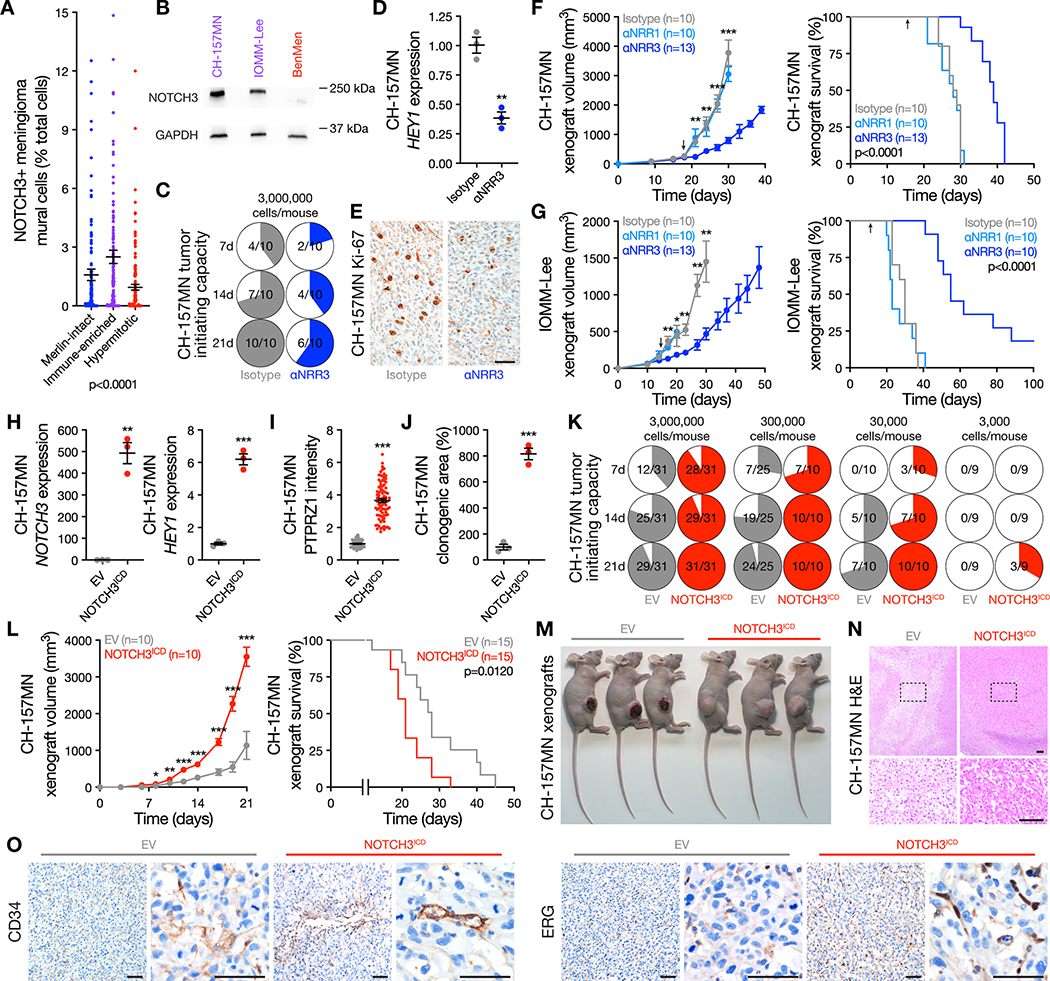
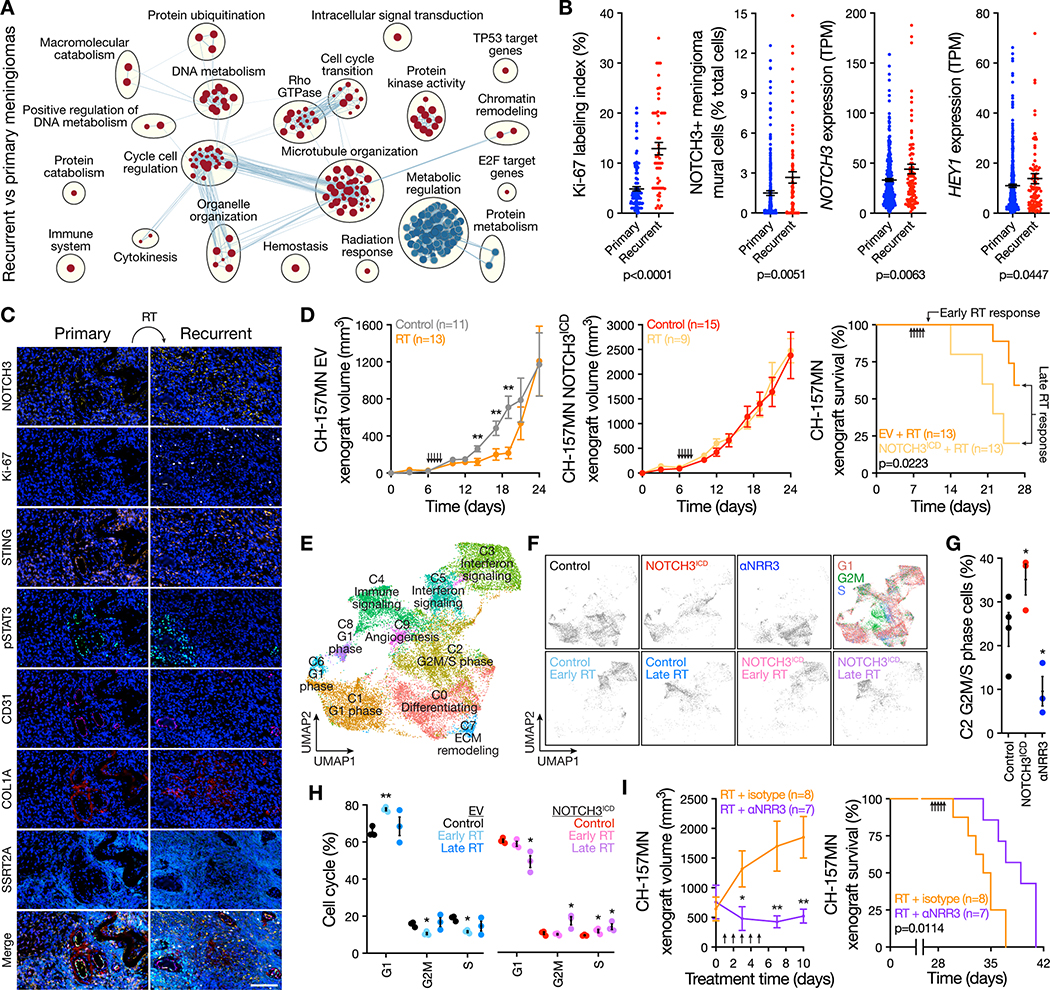
Meningiomas are the most common primary intracranial tumors. Treatments for patients with meningiomas are limited to surgery and radiotherapy, and systemic therapies remain ineffective or experimental. Resistance to radiotherapy is common in high-grade meningiomas and the cell types and signaling mechanisms that drive meningioma tumorigenesis and resistance to radiotherapy are incompletely understood. Here, we report that NOTCH3 drives meningioma tumorigenesis and resistance to radiotherapy and find that perivascular NOTCH3+ stem cells are conserved across meningiomas from humans, dogs, and mice. Integrating single-cell transcriptomics with lineage tracing and imaging approaches in genetically engineered mouse models and xenografts, we show NOTCH3 drives tumor-initiating capacity, cell proliferation, angiogenesis, and resistance to radiotherapy to increase meningioma growth and reduce survival. To translate these findings to patients, we show that an antibody stabilizing the extracellular negative regulatory region of NOTCH3 blocks meningioma tumorigenesis and sensitizes meningiomas to radiotherapy, reducing tumor growth and improving survival. Significance: There are no effective systemic therapies to treat meningiomas, and meningioma stem cells are poorly understood. Here, we report perivascular NOTCH3+ stem cells to drive meningioma tumorigenesis and resistance to radiotherapy. Our results identify a conserved mechanism and a therapeutic vulnerability to treat meningiomas that are resistant to standard interventions.
©2024 American Association for Cancer Research.
Conflict of interest statement
Conflict of interests statement
AA is a co-founder of Tango Therapeutics, Azkarra Therapeutics, Ovibio Corporation, and Kytarro; a member of the board of Cytomx and Cambridge Science Corporation; a member of the scientific advisory board of Genentech, GLAdiator, Circle, Bluestar, Earli, Ambagon, Phoenix Molecular Designs, Yingli, ProRavel, Oric, Hap10, and Trial Library; a consultant for SPARC, ProLynx, Novartis, and GSK; receives research support from SPARC; and holds patents on the use of PARP inhibitors held jointly with AstraZeneca.
Figures
Update of
-
NOTCH3 drives meningioma tumorigenesis and resistance to radiotherapy.bioRxiv [Preprint]. 2023 Jul 11:2023.07.10.548456. doi: 10.1101/2023.07.10.548456. bioRxiv. 2023. Update in: Cancer Discov. 2024 Oct 4;14(10):1823-1837. doi: 10.1158/2159-8290.CD-23-1459. PMID: 37503127 Free PMC article. Updated. Preprint.
Similar articles
-
NOTCH3 drives meningioma tumorigenesis and resistance to radiotherapy.bioRxiv [Preprint]. 2023 Jul 11:2023.07.10.548456. doi: 10.1101/2023.07.10.548456. bioRxiv. 2023. Update in: Cancer Discov. 2024 Oct 4;14(10):1823-1837. doi: 10.1158/2159-8290.CD-23-1459. PMID: 37503127 Free PMC article. Updated. Preprint.
-
KLF4 is a tumor suppressor in anaplastic meningioma stem-like cells and human meningiomas.J Mol Cell Biol. 2017 Aug 1;9(4):315-324. doi: 10.1093/jmcb/mjx023. J Mol Cell Biol. 2017. PMID: 28651379
-
Establishment and transcriptomic characteristics of radio-resistant meningioma cell lines.J Neurooncol. 2025 May;173(1):105-119. doi: 10.1007/s11060-025-04966-6. Epub 2025 Feb 28. J Neurooncol. 2025. PMID: 40019713
-
Intracranial meningiomas, the VEGF-A pathway, and peritumoral brain oedema.Dan Med J. 2013 Apr;60(4):B4626. Dan Med J. 2013. PMID: 23651727 Review.
-
Meta-analysis of adjuvant radiotherapy for intracranial atypical and malignant meningiomas.J Neurooncol. 2021 Apr;152(2):205-216. doi: 10.1007/s11060-020-03674-7. Epub 2021 Feb 26. J Neurooncol. 2021. PMID: 33635510 Review.
Cited by
-
Glioblastoma Phagocytic Cell Death: Balancing the Opportunities for Therapeutic Manipulation.Cells. 2024 May 11;13(10):823. doi: 10.3390/cells13100823. Cells. 2024. PMID: 38786045 Free PMC article. Review.
-
Interdisciplinary Therapeutic Approaches to Atypical and Malignant Meningiomas.Cancers (Basel). 2023 Aug 25;15(17):4251. doi: 10.3390/cancers15174251. Cancers (Basel). 2023. PMID: 37686527 Free PMC article. Review.
-
Single-cell analysis reveals a longitudinal trajectory of meningioma evolution and heterogeneity.Nat Commun. 2025 Jul 1;16(1):5481. doi: 10.1038/s41467-025-60653-0. Nat Commun. 2025. PMID: 40593590 Free PMC article.
-
Domestic Animal Models of Central Nervous System Tumors: Focus on Meningiomas.Life (Basel). 2023 Nov 30;13(12):2284. doi: 10.3390/life13122284. Life (Basel). 2023. PMID: 38137885 Free PMC article. Review.
-
Semi-automated approaches for interrogating spatial heterogeneity of tissue samples.Sci Rep. 2024 Feb 29;14(1):5025. doi: 10.1038/s41598-024-55387-w. Sci Rep. 2024. PMID: 38424144 Free PMC article.
References
-
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol [Internet]. 2021;23:1231–51. Available from: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id... - PMC - PubMed
-
- Simpson D The Recurrence of Intracranial Meningiomas After Surgical Treatment. J Neurosurg. 1957;58:51–56. Available from: http://books.google.com/books?id=YncCjwEACAAJ&dq=The+recurrence+of+intra... - PubMed
MeSH terms
Substances
Grants and funding
- R01 CA120813/CA/NCI NIH HHS/United States
- T32 GM007618/GM/NIGMS NIH HHS/United States
- CA262311/National Institutes of Health (NIH)
- F32 CA213944/CA/NCI NIH HHS/United States
- K08 NS116161/NS/NINDS NIH HHS/United States
- F30 CA246808/CA/NCI NIH HHS/United States
- DP2 MH136391/MH/NIMH NIH HHS/United States
- P50 CA097257/CA/NCI NIH HHS/United States
- R01 NS118039/NS/NINDS NIH HHS/United States
- R01 NS120547/NS/NINDS NIH HHS/United States
- R01 NS117104/NS/NINDS NIH HHS/United States
- R01 CA262311/CA/NCI NIH HHS/United States
- P50 CA221747/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
