

Construction and validation of nomogram model for predicting the risk of ventricular arrhythmia after emergency PCI in patients with acute myocardial infarction
- PMID: 38742959
- PMCID: PMC11132015
- DOI: 10.18632/aging.205815
Construction and validation of nomogram model for predicting the risk of ventricular arrhythmia after emergency PCI in patients with acute myocardial infarction
Abstract
Objective: To make predictions about the risk of MVA (Malignant Ventricular Arrhythmia) after primary PCI (Percutaneous Coronary Intervention) in patients with AMI (Acute Myocardial Infarction) through constructing and validating the Nomogram model.
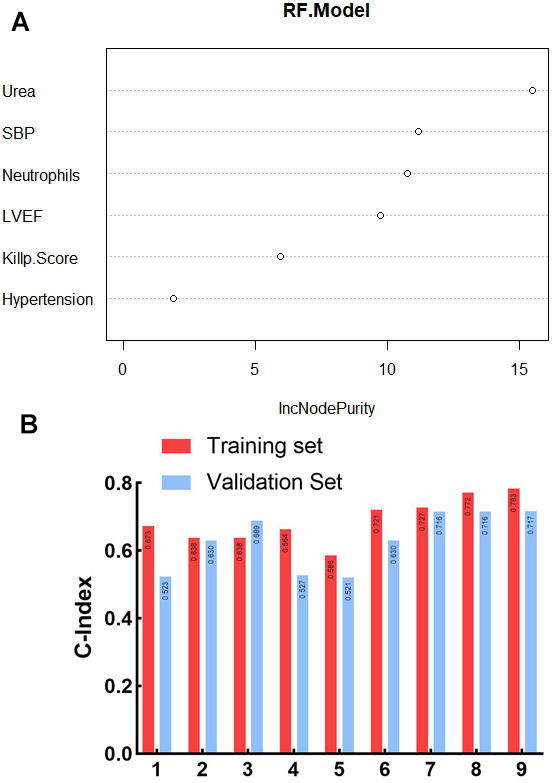
Methods: 311 AMI patients who suffered from emergency PCI in Hefei Second People's Hospital from January 2020 to May 2023 were selected as the training set; 253 patients suffering from the same symptom in Hefei First People's Hospital during the same period were selected as the validation set. Risk factors were further screened by means of multivariate logistic and stepwise regression. The nomogram model was constructed, and then validated by using C-index, ROC curve, decision curve and calibration curve.
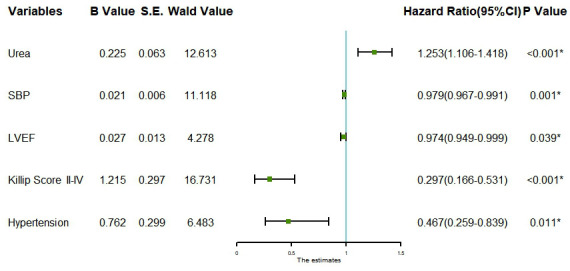
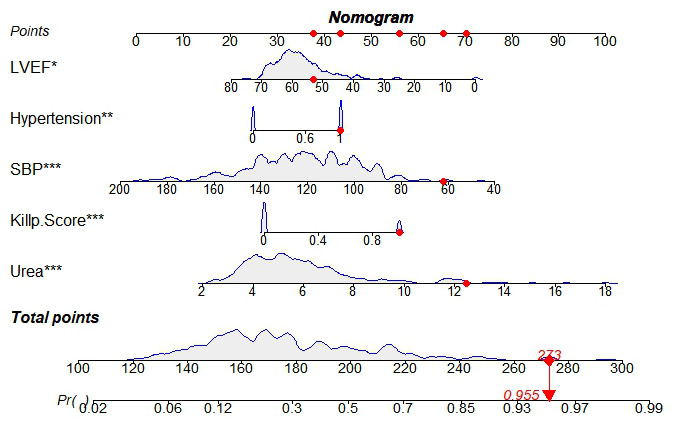
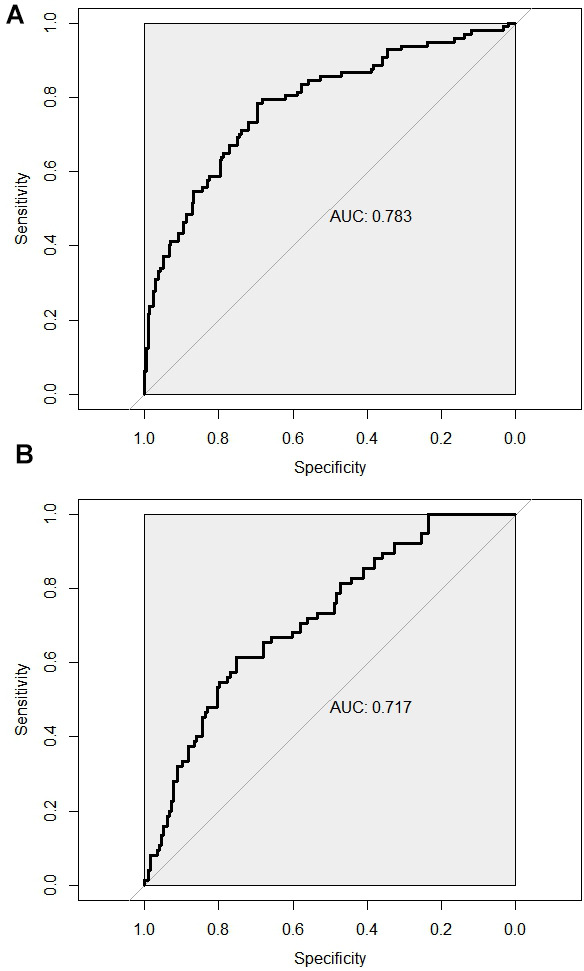
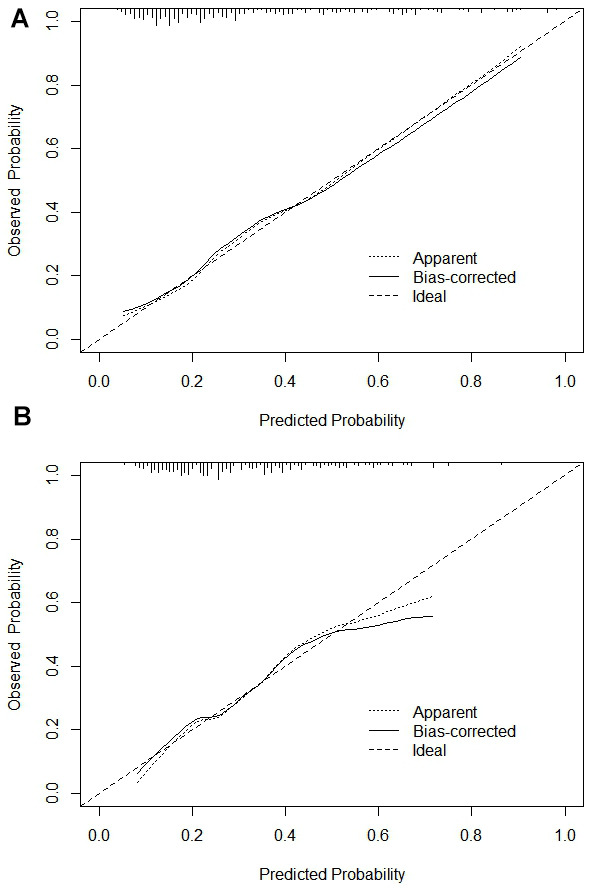
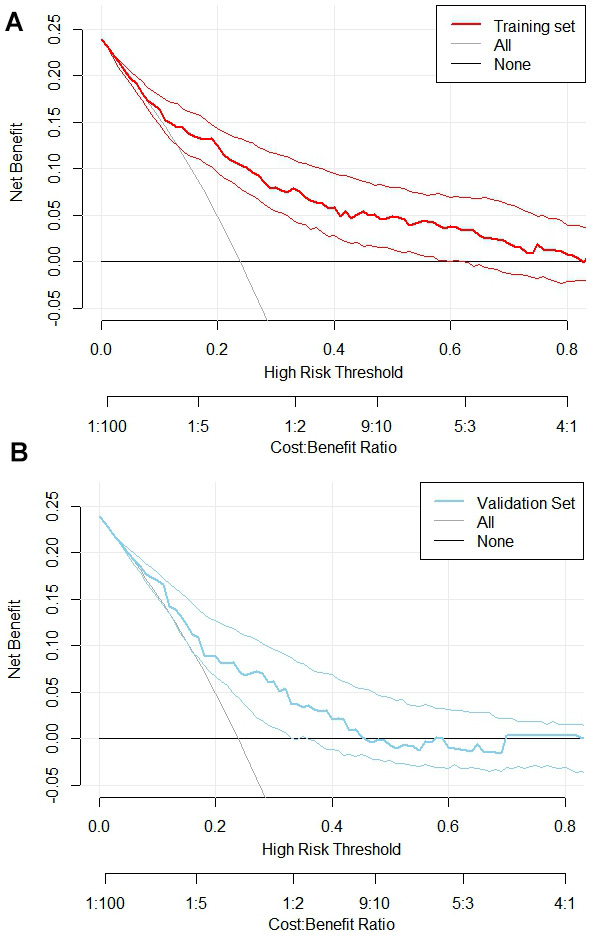
Results: Multivariate logistic analysis revealed that urea, systolic pressure, hypertension, Killip class II-IV, as well as LVEF (Left Ventricular Ejection Fraction) were all unrelated hazards for MVA after emergency PCI for AMI (P<0.05); a risk prediction nomogram model was constructed. The C-index was calculated to evaluate the predictive ability of the model. Result showed that the index of the training and the validation set was 0.783 (95% CI: 0.726-0.84) and 0.717 (95% CI: 0.65-0.784) respectively, which suggested that the model discriminated well. Meanwhile, other tools including ROC curve, calibration curve and decision curve also proved that this nomogram plays an effective role in forecasting the risk for MVA after PCI in AMI patients.
Conclusions: The study successfully built the nomogram model and made predictions for the development of MVA after PCI in AMI patients.
Keywords: AMI (acute myocardial infarction); PCI (percutaneous coronary intervention); predictive model; ventricular arrhythmia.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
