

Prevalence and location of coronary artery disease in anomalous aortic origin of coronary arteries
- PMID: 38742995
- PMCID: PMC11524620
- DOI: 10.1097/MCA.0000000000001385
Prevalence and location of coronary artery disease in anomalous aortic origin of coronary arteries
Abstract
Background: The prevalence and location of coronary artery disease (CAD) in anomalous aortic origin of a coronary artery (AAOCA) remain poorly documented in adults. We sought to assess the presence of CAD in proximal (or ectopic) and distal (or nonectopic) segments of AAOCA. We hypothesized that the representation of CAD may differ among the different courses of AAOCA.
Methods: The presence of CAD was analyzed on coronary angiography and/or coronary computed tomography angiography in 390 patients (median age 64 years; 73% male) with AAOCA included in the anomalous coronary arteries multicentric registry.
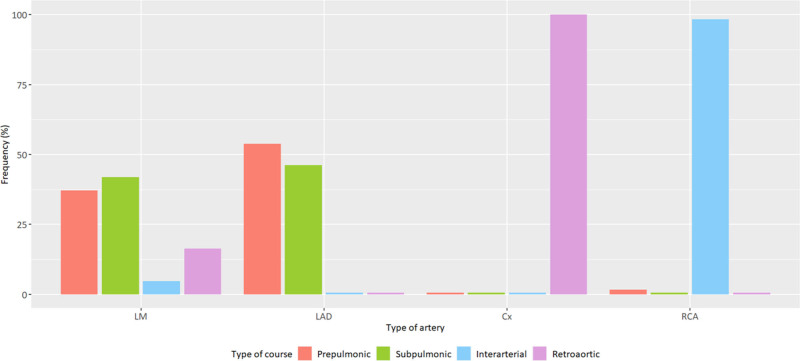
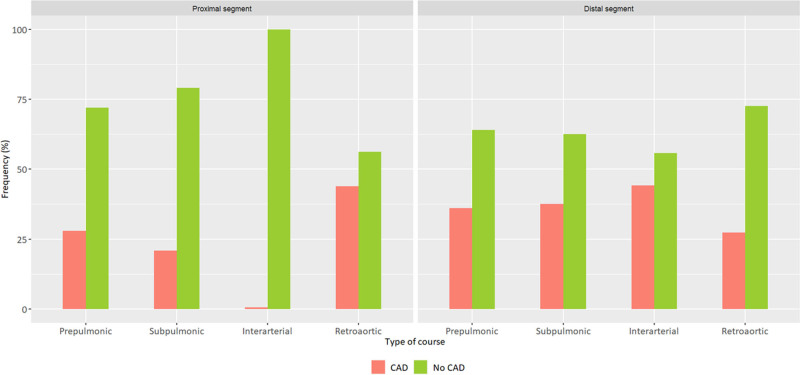
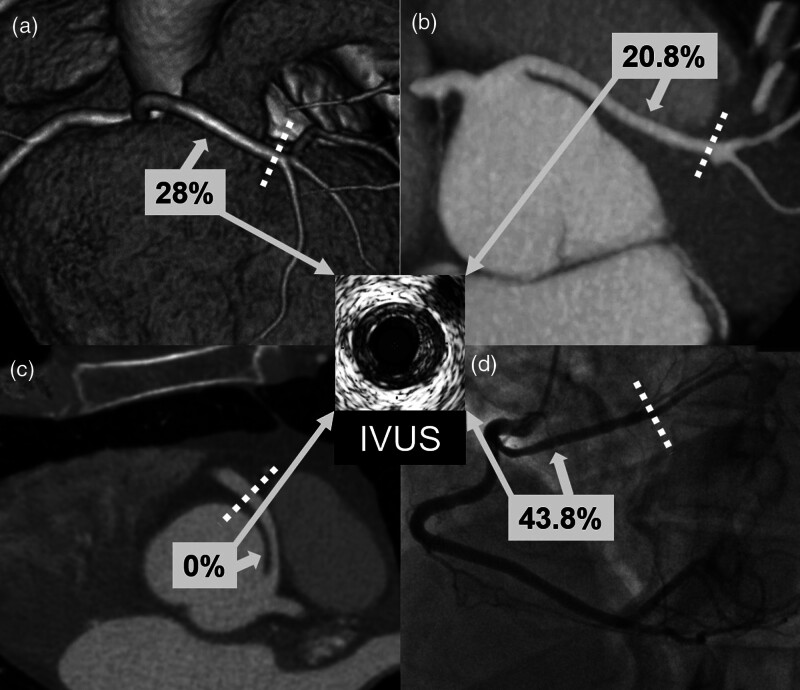
Results: AAOCA mainly involved circumflex artery (54.4%) and right coronary artery (RCA) (31.3%). All circumflex arteries had a retroaortic course; RCA mostly an interarterial course (98.4%). No CAD was found in the proximal segment of interarterial AAOCA, whereas 43.8% of retroaortic AAOCA, 28% of prepulmonic AAOCA and 20.8% subpulmonic AAOCA had CAD in their proximal segments ( P < 0.001). CAD was more prevalent in proximal than in distal segments of retroaortic AAOCA (OR: 3.1, 95% CI: 1.8-5.4, P < 0.001). On multivariate analysis, a retroaortic course was associated with an increased prevalence of CAD in the proximal segment (adjusted OR 3.4, 95% CI: 1.3-10.7, P = 0.022).
Conclusion: Increased prevalence of CAD was found in the proximal segment of retroaortic AAOCA compared to the proximal segments of other AAOCA, whereas no CAD was observed in the proximal segment of interarterial AAOCA. The mechanisms underlying these differences are not yet clearly identified.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Cheezum MK, Liberthson RR, Shah NR, Villines TC, O’Gara PT, Lanszberg MJ, et al. Anomalous aortic origin of a coronary artery from the inappropriate sinus of valsalva. J Am Coll Cardiol 2017; 69:1592–1608. - PubMed
-
- Chaitman BR, Lespérance J, Saltiel J, Bourassa MB. Clinical, angiographic, and hemodynamic findings in patients with anomalous origin of the coronary arteries. Circulation 1976; 53:122–131. - PubMed
-
- Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol 1992; 34:129–138. - PubMed
-
- Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study. Int J Cardiol 2000; 74:39–46. - PubMed
-
- Jim MH, Siu CW, Ho HH, Miu R, Lee SW. Anomalous origin of the right coronary artery from the left coronary sinus is associated with early development of coronary artery disease. J Invasive Cardiol 2004; 16:466–468. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
