

Harm-to-self from gambling: A national study of Australian adults
- PMID: 38743487
- PMCID: PMC11220818
- DOI: 10.1556/2006.2024.00025
Harm-to-self from gambling: A national study of Australian adults
Abstract
Aims: Understanding how gambling harm is distributed is essential to inform effective harm reduction measures. This first national Australian study of gambling harm-to-self examined the extent, distribution, risk factors, and health related quality of life (HRQoL) impacts of this harm.
Methods: A Random Digit Dialling sample of 15,000 Australian adults was weighted to key population variables. Key measures included the Gambling Harms Scale-10 (GHS-10), PGSI, SF-6D, gambling behaviours, and demographics. Analyses included ordinal logistic regression.
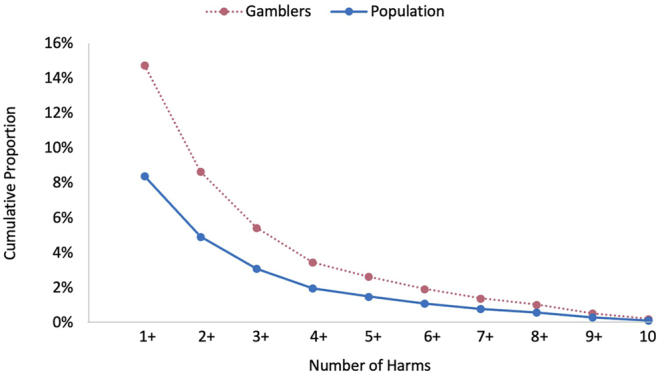
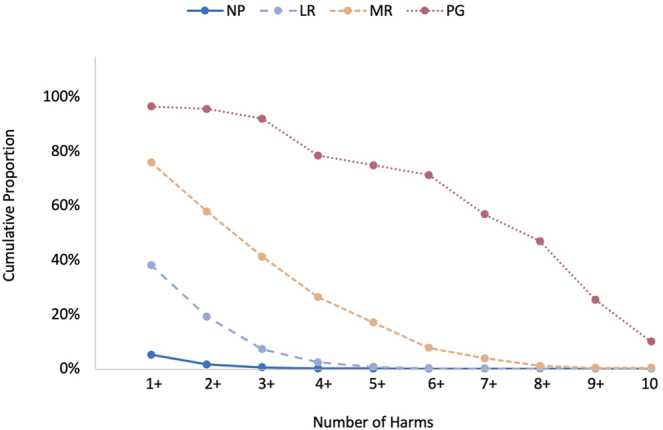
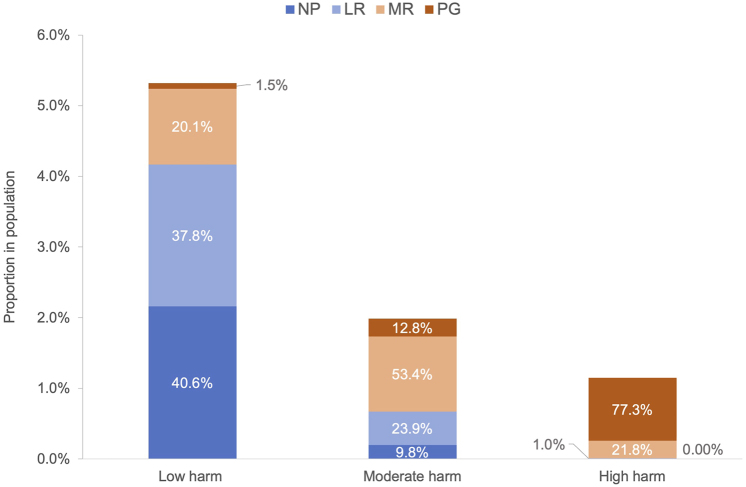
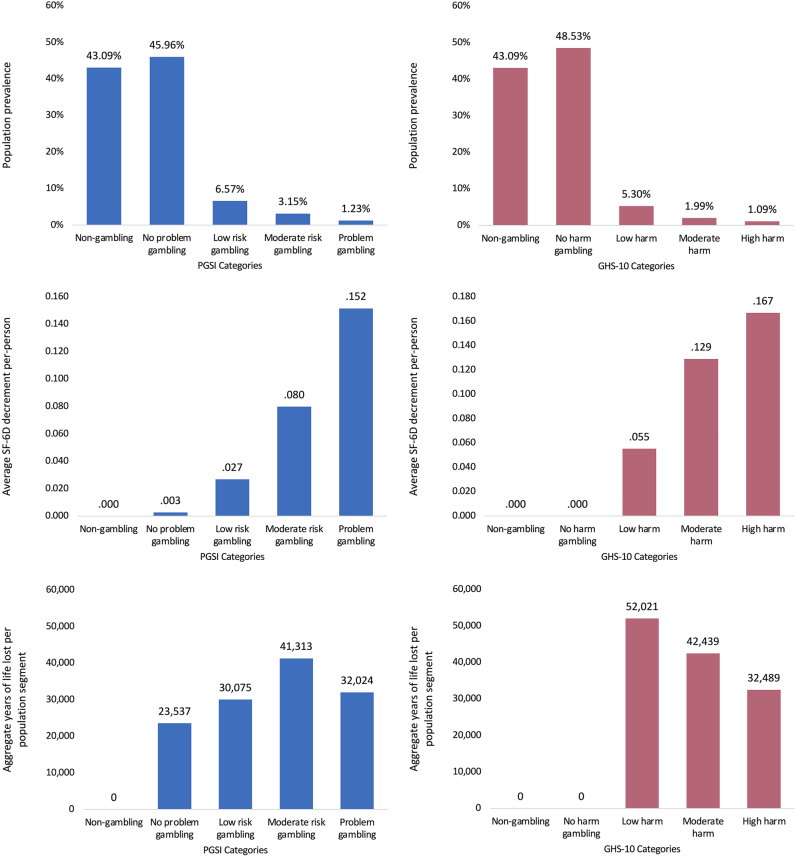
Results: Amongst gamblers, 14.7% reported harm on the GHS-10, including 1.9% reporting high-level harm. While high-level harm occurred mainly in the problem gambling group (77.3%), other PGSI groups accounted for most of the more prevalent low (98.5%) and moderate (87.2%) harms reported. Proximal predictors of greater harm were use of online gambling and more frequent gambling on electronic gaming machines (EGMs), race betting sports betting, poker, skin gambling, scratchies, and loot box purchasing. Distal predictors were being younger, male, single, Aboriginal or Torres Strait Islander, and speaking a non-English language at home. At the population level, the greatest aggregate HRQoL impacts were amongst lower-risk gamblers, confirming the results of other studies regarding the 'prevention paradox'.
Conclusions: The distribution of harm across gambler risk groups indicates the need for preventive measures, not just interventions for problem gambling. Reducing harm requires modifying product features that amplify their risk, especially for EGMs, race betting and sports betting that are both inherently risky and widely used. Gambling harm exacerbates health disparities for disadvantaged and vulnerable groups, requiring targeted resources and support.
Keywords: gambling harm; gambling products; health-related quality of life (HRQoL) population study; health inequity; risk factors.
Conflict of interest statement
Figures
References
-
- ACIL Allen Consulting, Deakin University (Dowling, A. & Merkouris, S.), Central Queensland University (Browne, M. & Rockloff, M.), & the Social Research Centre (2018). Fourth social and economic impact study of gambling in Tasmania: Report 2. Hobart: Tasmanian Department of Treasury and Finance. https://www.acilallen.com.au/projects/other/fourth-social-and-economic-i....
-
- Afifi, T. O., LaPlante, D. A., Taillieu, T. L., Dowd, D., & Shaffer, H. J. (2014). Gambling involvement: Considering frequency of play and the moderating effects of gender and age. International Journal of Mental Health and Addiction, 12, 283–294. 10.1007/s11469-013-9452-3. - DOI
-
- American Association for Public Opinion Research (2017). The future of U.S. general population telephone survey research. Retrieved from https://www.aapor.org/getattachment/Education-Resources/Reports/Future-o....
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
