

IL-7-primed bystander CD8 tumor-infiltrating lymphocytes optimize the antitumor efficacy of T cell engager immunotherapy
- PMID: 38744277
- PMCID: PMC11148861
- DOI: 10.1016/j.xcrm.2024.101567
IL-7-primed bystander CD8 tumor-infiltrating lymphocytes optimize the antitumor efficacy of T cell engager immunotherapy
Abstract
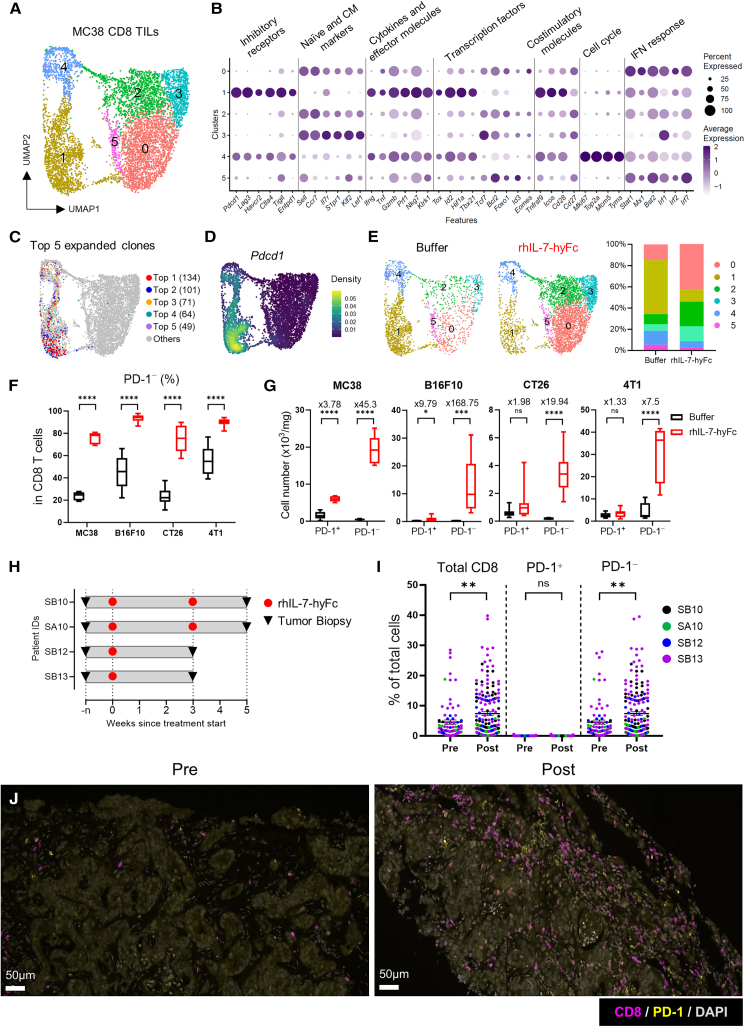
Bispecific T cell engagers (TCEs) show promising clinical efficacy in blood tumors, but their application to solid tumors remains challenging. Here, we show that Fc-fused IL-7 (rhIL-7-hyFc) changes the intratumoral CD8 T cell landscape, enhancing the efficacy of TCE immunotherapy. rhIL-7-hyFc induces a dramatic increase in CD8 tumor-infiltrating lymphocytes (TILs) in various solid tumors, but the majority of these cells are PD-1-negative tumor non-responsive bystander T cells. However, they are non-exhausted and central memory-phenotype CD8 T cells with high T cell receptor (TCR)-recall capacity that can be triggered by tumor antigen-specific TCEs to acquire tumoricidal activity. Single-cell transcriptome analysis reveals that rhIL-7-hyFc-induced bystander CD8 TILs transform into cycling transitional T cells by TCE redirection with decreased memory markers and increased cytotoxic molecules. Notably, TCE treatment has no major effect on tumor-reactive CD8 TILs. Our results suggest that rhIL-7-hyFc treatment promotes the antitumor efficacy of TCE immunotherapy by increasing TCE-sensitive bystander CD8 TILs in solid tumors.
Keywords: bispecific T cell engager; bystander CD8 T cell; cancer immunotherapy; combination therapy; interleukin-7; solid tumors; tumor microenvironment; tumor-infiltrating lymphocytes.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests M.L., S.-K.I., and D.C. are employees of the Research Institute of NeoImmuneTech, Inc., which supports the supply of rhIL-7-hyFc and its formulation buffer.
Figures






References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
