

A burden of proof study on alcohol consumption and ischemic heart disease
- PMID: 38744810
- PMCID: PMC11094064
- DOI: 10.1038/s41467-024-47632-7
A burden of proof study on alcohol consumption and ischemic heart disease
Abstract
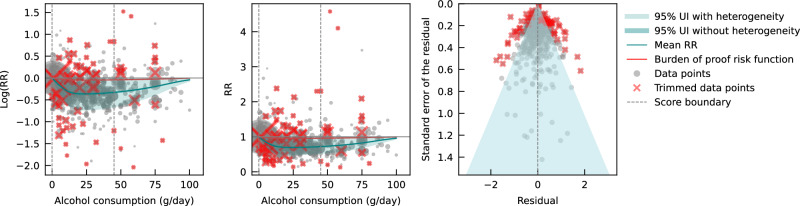
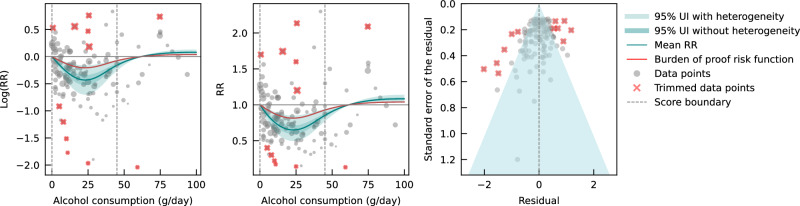
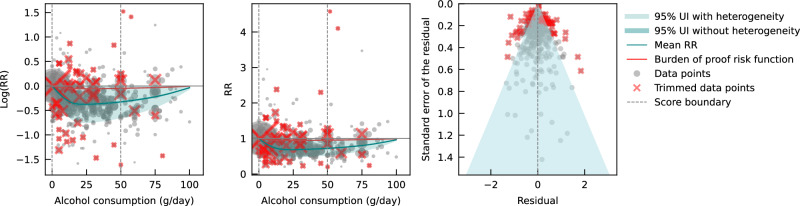
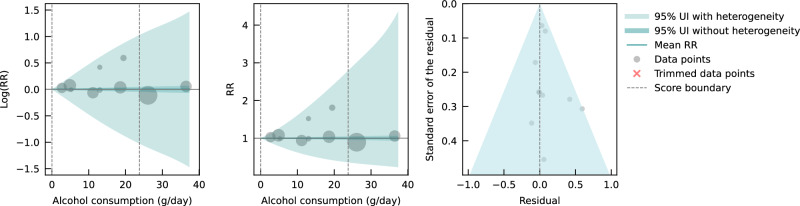
Cohort and case-control data have suggested an association between low to moderate alcohol consumption and decreased risk of ischemic heart disease (IHD), yet results from Mendelian randomization (MR) studies designed to reduce bias have shown either no or a harmful association. Here we conducted an updated systematic review and re-evaluated existing cohort, case-control, and MR data using the burden of proof meta-analytical framework. Cohort and case-control data show low to moderate alcohol consumption is associated with decreased IHD risk - specifically, intake is inversely related to IHD and myocardial infarction morbidity in both sexes and IHD mortality in males - while pooled MR data show no association, confirming that self-reported versus genetically predicted alcohol use data yield conflicting findings about the alcohol-IHD relationship. Our results highlight the need to advance MR methodologies and emulate randomized trials using large observational databases to obtain more definitive answers to this critical public health question.
© 2024. The Author(s).
Conflict of interest statement
G.A.R. has received support for this manuscript from the Bill and Melinda Gates Foundation [OPP1152504]. S.L. has received grants or contracts from the UK Medical Research Council [MR/T017708/1], CDC Foundation [project number 996], World Health Organization [APW No 2021/1194512], and is affiliated with the NIHR Oxford Biomedical Research Centre. The University of Oxford’s Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU) is supported by core grants from the Medical Research Council [Clinical Trial Service Unit A310] and the British Heart Foundation [CH/1996001/9454]. The CTSU receives research grants from industry that are governed by University of Oxford contracts that protect its independence and has a staff policy of not taking personal payments from industry. All other authors declare no competing interests.
Figures
Similar articles
-
Milk intake is not associated with ischaemic heart disease in observational or Mendelian randomization analyses in 98,529 Danish adults.Int J Epidemiol. 2015 Apr;44(2):587-603. doi: 10.1093/ije/dyv109. Int J Epidemiol. 2015. PMID: 26085675
-
Ischemic heart disease mortality and morbidity rates in former drinkers: a meta-analysis.Am J Epidemiol. 2011 Feb 1;173(3):245-58. doi: 10.1093/aje/kwq364. Epub 2010 Dec 14. Am J Epidemiol. 2011. PMID: 21156750 Free PMC article.
-
The effect of exposure to long working hours on ischaemic heart disease: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury.Environ Int. 2020 Sep;142:105739. doi: 10.1016/j.envint.2020.105739. Epub 2020 Jun 5. Environ Int. 2020. PMID: 32505014 Free PMC article.
-
Differential Associations of Alcohol Use With Ischemic Heart Disease Mortality by Socioeconomic Status in the US, 1997-2018.JAMA Netw Open. 2024 Feb 5;7(2):e2354270. doi: 10.1001/jamanetworkopen.2023.54270. JAMA Netw Open. 2024. PMID: 38300620 Free PMC article.
-
The effect of exposure to long working hours on alcohol consumption, risky drinking and alcohol use disorder: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury.Environ Int. 2021 Jan;146:106205. doi: 10.1016/j.envint.2020.106205. Epub 2020 Nov 12. Environ Int. 2021. PMID: 33189992 Free PMC article.
Cited by
-
A systematic review with a Burden of Proof meta-analysis of health effects of long-term ambient fine particulate matter (PM2.5) exposure on dementia.Nat Aging. 2025 May;5(5):897-908. doi: 10.1038/s43587-025-00844-y. Epub 2025 Mar 21. Nat Aging. 2025. PMID: 40119171 Free PMC article.
-
The Impact of Alcohol on Sleep Physiology: A Prospective Observational Study on Nocturnal Resting Heart Rate Using Smartwatch Technology.Nutrients. 2025 Apr 26;17(9):1470. doi: 10.3390/nu17091470. Nutrients. 2025. PMID: 40362779 Free PMC article.
-
Global, regional, and national burden and risk factors of ischemic heart disease, 1990-2021: an analysis of the global burden of disease study.Front Public Health. 2025 Apr 25;13:1563631. doi: 10.3389/fpubh.2025.1563631. eCollection 2025. Front Public Health. 2025. PMID: 40352854 Free PMC article.
-
A flavonoid-rich diet is associated with lower risk and improved imaging biomarkers of nonalcoholic fatty liver disease: a prospective cohort study.Am J Clin Nutr. 2024 Dec;120(6):1325-1334. doi: 10.1016/j.ajcnut.2024.09.022. Epub 2024 Sep 26. Am J Clin Nutr. 2024. PMID: 39341459 Free PMC article.
-
Global, regional, and national burden of ischemic heart disease attributable to metabolic risks: a systematic analysis of Global Burden of Disease 2021.J Geriatr Cardiol. 2025 Mar 28;22(3):361-380. doi: 10.26599/1671-5411.2025.03.009. J Geriatr Cardiol. 2025. PMID: 40351395 Free PMC article.
References
-
- World Health Organization. Global Status Report on Alcohol and Health 2018. (World Health Organization, Geneva, Switzerland, 2019).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
