

Distinct cytokine profiles in late pregnancy in Ugandan people with HIV
- PMID: 38744864
- PMCID: PMC11093984
- DOI: 10.1038/s41598-024-61764-2
Distinct cytokine profiles in late pregnancy in Ugandan people with HIV
Abstract
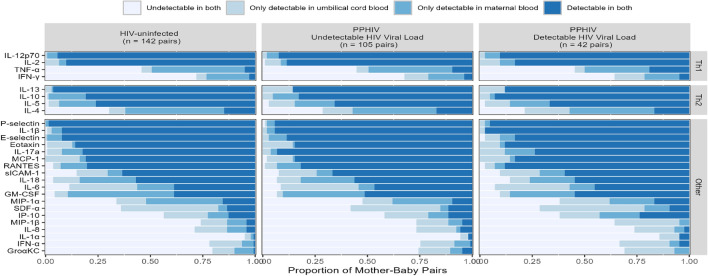
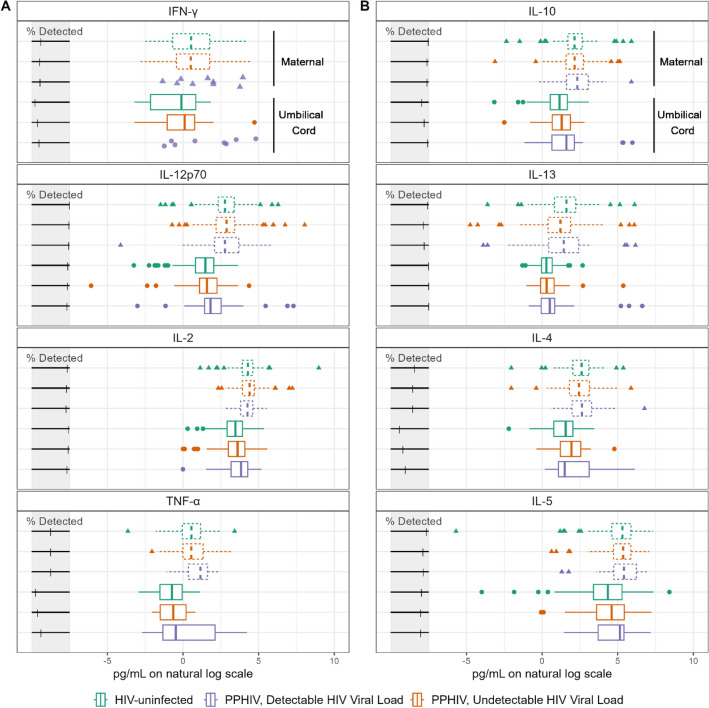
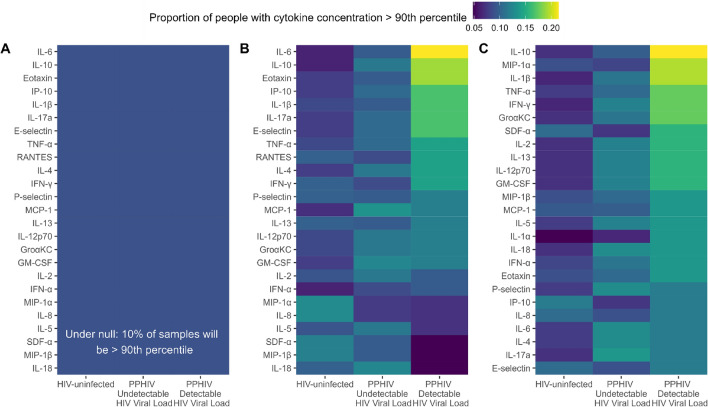
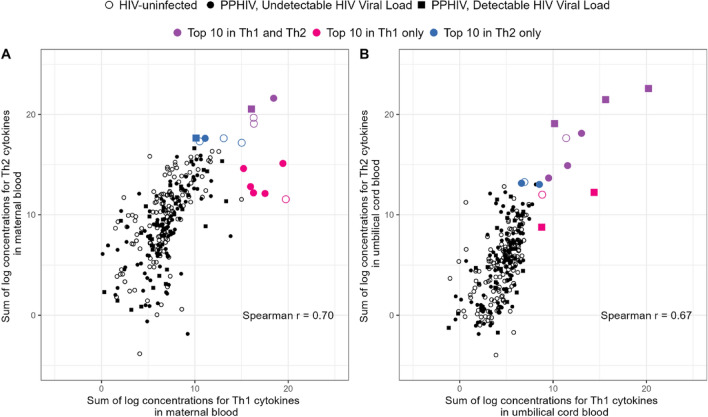
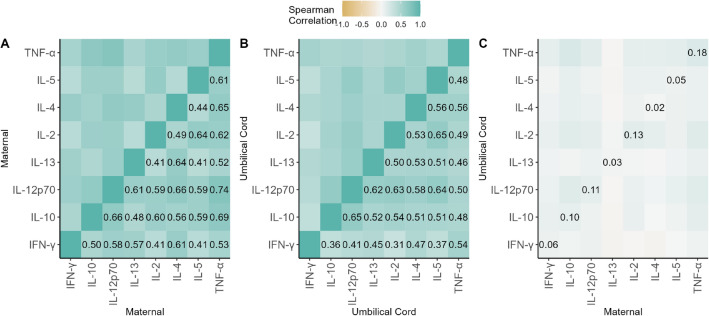
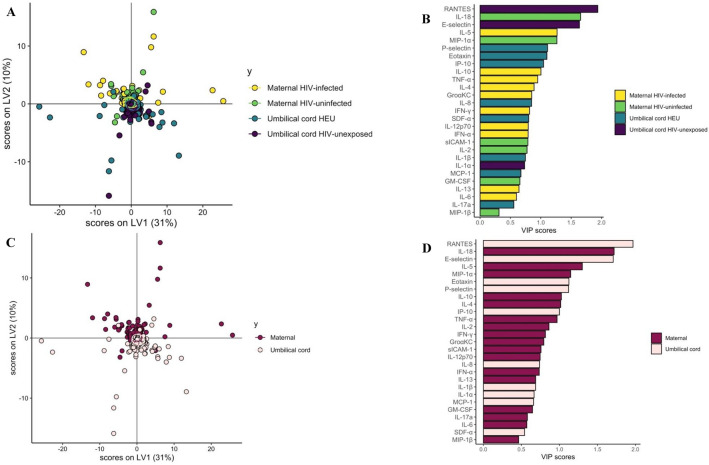
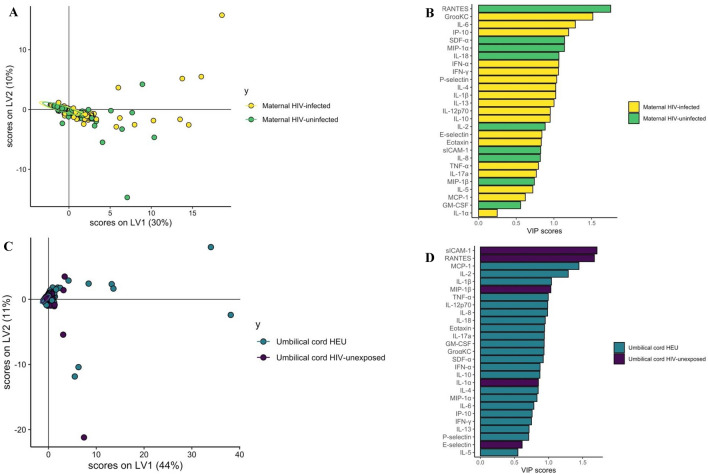
During pregnancy, multiple immune regulatory mechanisms establish an immune-tolerant environment for the allogeneic fetus, including cellular signals called cytokines that modify immune responses. However, the impact of maternal HIV infection on these responses is incompletely characterized. We analyzed paired maternal and umbilical cord plasma collected during labor from 147 people with HIV taking antiretroviral therapy and 142 HIV-uninfected comparators. Though cytokine concentrations were overall similar between groups, using Partial Least Squares Discriminant Analysis we identified distinct cytokine profiles in each group, driven by higher IL-5 and lower IL-8 and MIP-1α levels in pregnant people with HIV and higher RANTES and E-selectin in HIV-unexposed umbilical cord plasma (P-value < 0.01). Furthermore, maternal RANTES, SDF-α, gro -KC, IL-6, and IP-10 levels differed significantly by HIV serostatus (P < 0.01). Although global maternal and umbilical cord cytokine profiles differed significantly (P < 0.01), umbilical cord plasma profiles were similar by maternal HIV serostatus. We demonstrate that HIV infection is associated with a distinct maternal plasma cytokine profile which is not transferred across the placenta, indicating a placental role in coordinating local inflammatory response. Furthermore, maternal cytokine profiles in people with HIV suggest an incomplete shift from Th2 to Th1 immune phenotype at the end of pregnancy.
© 2024. The Author(s).
Conflict of interest statement
GA is a V.P. at Moderna, a founder and equity holder of Seromyx Systems, and an employee and equity holder of Leyden Labs. GA’s interests were reviewed and are managed by MGH and Partners HealthCare in accordance with their conflict-of-interest policies. All other authors declare that they have no competing interests.
Figures
References
-
- Schoeman JC, Moutloatse GP, Harms AC, et al. Fetal metabolic stress disrupts immune homeostasis and induces proinflammatory responses in human immunodeficiency virus type 1- and combination antiretroviral therapy-exposed infants. J. Infect. Dis. 2017;216(4):436–446. doi: 10.1093/infdis/jix291. - DOI - PMC - PubMed
MeSH terms
Grants and funding
- KL2 TR002542/TR/NCATS NIH HHS/United States
- K24AI141036/National Institute of Allergy and Infectious Diseases
- K23AI138856/National Institute of Allergy and Infectious Diseases
- 3R37AI080289-11S1/National Institute of Allergy and Infectious Diseases
- R01 AI146785/AI/NIAID NIH HHS/United States
- Burroughs Wellcome Postdoctoral Fellowship in Tropical Infectious Diseases/American Society of Tropical Medicine and Hygiene
- P30AI060354/Harvard University Center for AIDS Research
- KL2TR002542/Harvard Catalyst
- P30 AI060354/AI/NIAID NIH HHS/United States
- K23 AI138856/AI/NIAID NIH HHS/United States
- R01AI146785/National Institute of Allergy and Infectious Diseases,United States
- U01 CA260476/CA/NCI NIH HHS/United States
- R37 AI080289/AI/NIAID NIH HHS/United States
- K24 AI141036/AI/NIAID NIH HHS/United States
- CIVIC75N93019C0005/Civic
LinkOut - more resources
Full Text Sources
Medical
