

A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis
- PMID: 38744955
- PMCID: PMC11094047
- DOI: 10.1038/s41746-024-01103-x
A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis
Erratum in
-
Author Correction: A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis.NPJ Digit Med. 2024 May 24;7(1):141. doi: 10.1038/s41746-024-01138-0. NPJ Digit Med. 2024. PMID: 38789723 Free PMC article. No abstract available.
Abstract
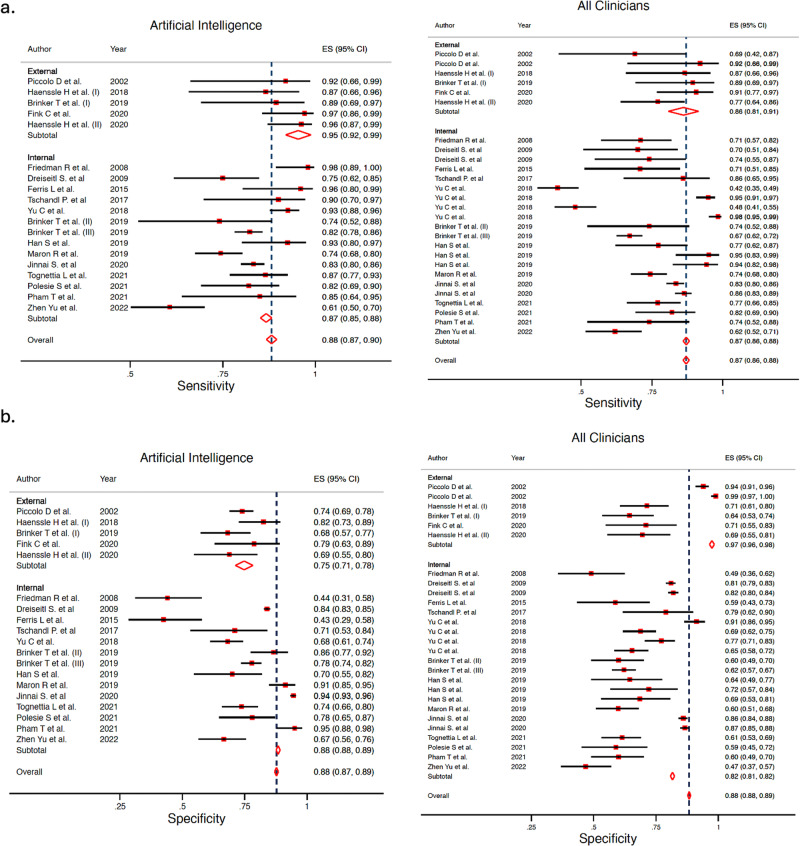
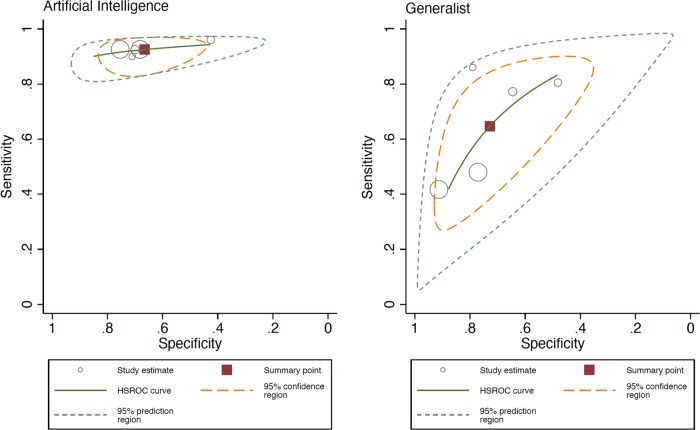
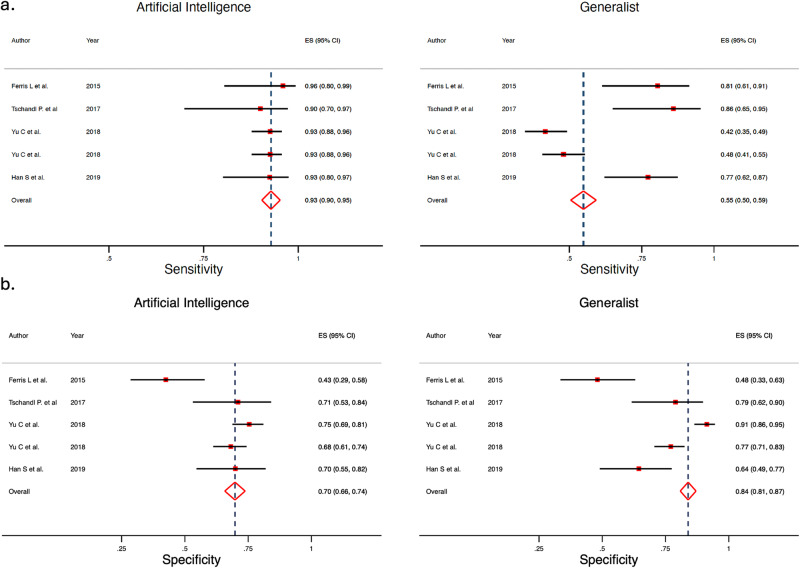
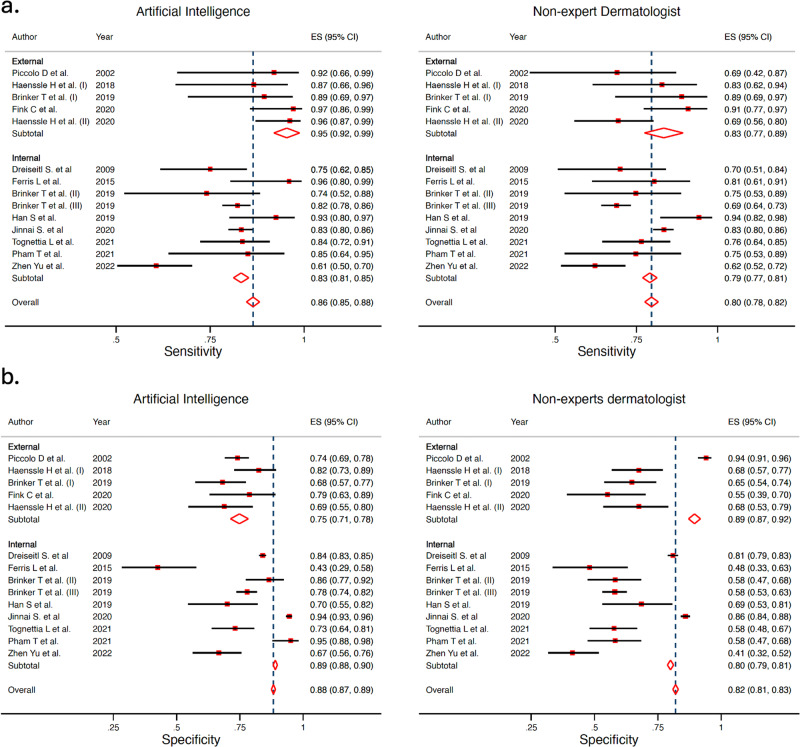
Scientific research of artificial intelligence (AI) in dermatology has increased exponentially. The objective of this study was to perform a systematic review and meta-analysis to evaluate the performance of AI algorithms for skin cancer classification in comparison to clinicians with different levels of expertise. Based on PRISMA guidelines, 3 electronic databases (PubMed, Embase, and Cochrane Library) were screened for relevant articles up to August 2022. The quality of the studies was assessed using QUADAS-2. A meta-analysis of sensitivity and specificity was performed for the accuracy of AI and clinicians. Fifty-three studies were included in the systematic review, and 19 met the inclusion criteria for the meta-analysis. Considering all studies and all subgroups of clinicians, we found a sensitivity (Sn) and specificity (Sp) of 87.0% and 77.1% for AI algorithms, respectively, and a Sn of 79.78% and Sp of 73.6% for all clinicians (overall); differences were statistically significant for both Sn and Sp. The difference between AI performance (Sn 92.5%, Sp 66.5%) vs. generalists (Sn 64.6%, Sp 72.8%), was greater, when compared with expert clinicians. Performance between AI algorithms (Sn 86.3%, Sp 78.4%) vs expert dermatologists (Sn 84.2%, Sp 74.4%) was clinically comparable. Limitations of AI algorithms in clinical practice should be considered, and future studies should focus on real-world settings, and towards AI-assistance.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
-
- Sangers, T. E. et al. Position statement of the EADV Artificial Intelligence (AI) Task Force on AI-assisted smartphone apps and web-based services for skin disease. J. Eur. Acad. Dermatol Venereol10.1111/jdv.19521 (2023). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
