

Prognostic relevance of radiological findings on early postoperative MRI for 187 consecutive glioblastoma patients receiving standard therapy
- PMID: 38744979
- PMCID: PMC11094076
- DOI: 10.1038/s41598-024-61925-3
Prognostic relevance of radiological findings on early postoperative MRI for 187 consecutive glioblastoma patients receiving standard therapy
Abstract
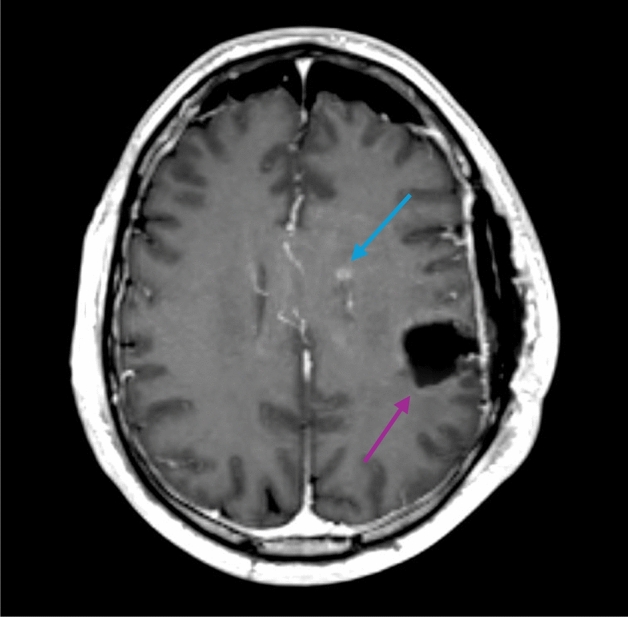
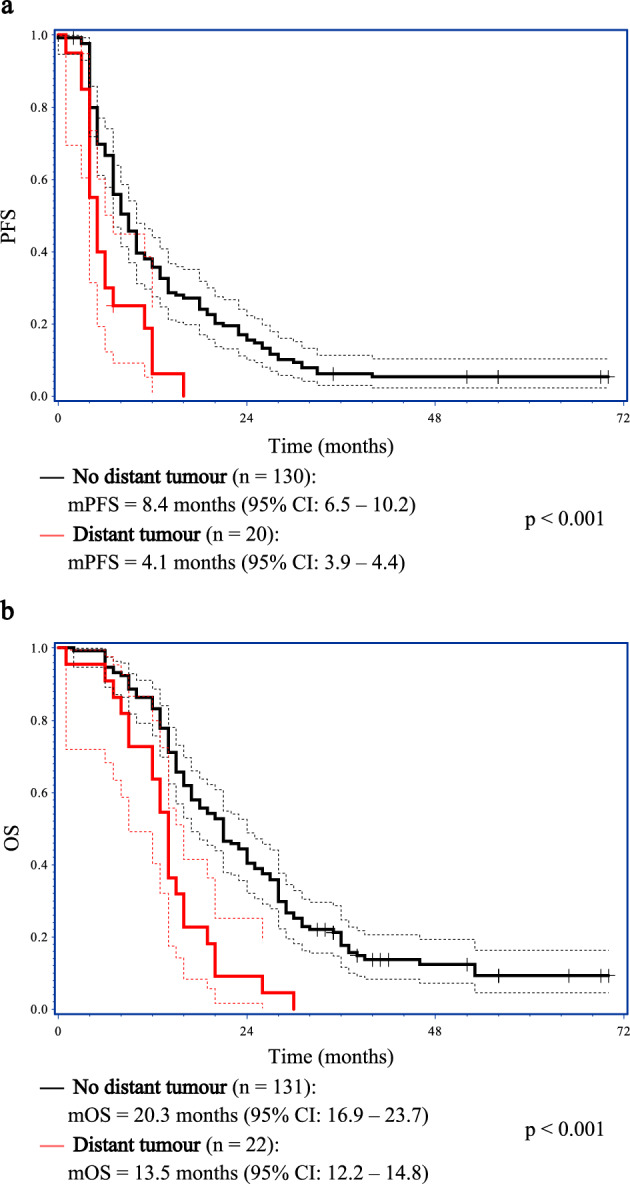
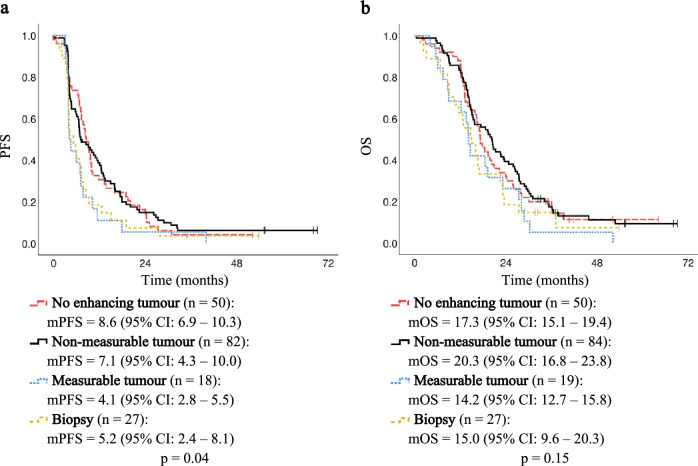
Several prognostic factors are known to influence survival for patients treated with IDH-wildtype glioblastoma, but unknown factors may remain. We aimed to investigate the prognostic implications of early postoperative MRI findings. A total of 187 glioblastoma patients treated with standard therapy were consecutively included. Patients either underwent a biopsy or surgery followed by an early postoperative MRI. Progression-free survival (PFS) and overall survival (OS) were analysed for known prognostic factors and MRI-derived candidate factors: resection status as defined by the response assessment in neuro-oncology (RANO)-working group (no contrast-enhancing residual tumour, non-measurable contrast-enhancing residual tumour, or measurable contrast-enhancing residual tumour) with biopsy as reference, contrast enhancement patterns (no enhancement, thin linear, thick linear, diffuse, nodular), and the presence of distant tumours. In the multivariate analysis, patients with no contrast-enhancing residual tumour or non-measurable contrast-enhancing residual tumour on the early postoperative MRI displayed a significantly improved progression-free survival compared with patients receiving only a biopsy. Only patients with non-measurable contrast-enhancing residual tumour showed improved overall survival in the multivariate analysis. Contrast enhancement patterns were not associated with survival. The presence of distant tumours was significantly associated with both poor progression-free survival and overall survival and should be considered incorporated into prognostic models.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
