

Adverse events associated with immune checkpoint inhibitors in non-small cell lung cancer: a safety analysis of clinical trials and FDA pharmacovigilance system
- PMID: 38745663
- PMCID: PMC11091284
- DOI: 10.3389/fimmu.2024.1396752
Adverse events associated with immune checkpoint inhibitors in non-small cell lung cancer: a safety analysis of clinical trials and FDA pharmacovigilance system
Abstract
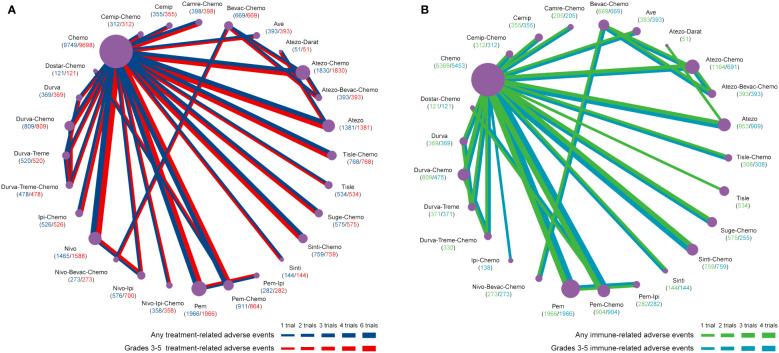
Objectives: Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of non-small cell lung cancer (NSCLC). However, the application of ICIs can also cause treatment-related adverse events (trAEs) and immune-related adverse events (irAEs). This study was to evaluate both the irAEs and trAEs of different ICI strategies for NSCLC based on randomized clinical trials (RCTs). The study also examined real-world pharmacovigilance data from the Food and Drug Administration Adverse Event Reporting System (FAERS) regarding claimed ICI-associated AEs in clinical practice.
Methods: Based on Pubmed, Embase, Medline, and the Cochrane CENTRAL, we retrieved RCTs comparing ICIs with chemotherapy drugs or with different ICI regimens for the treatment of NSCLC up to October 20, 2023. Bayesian network meta-analysis (NMA) was performed using odds ratios (ORs) with 95% credible intervals (95%CrI). Separately, a retrospective pharmacovigilance study was performed based on FAERS database, extracting ICI-associated AEs in NSCLC patients between the first quarter (Q1) of 2004 and Q4 of 2023. The proportional reports reporting odds ratio was calculated to analyze the disproportionality.
Results: The NMA included 51 RCTs that involved a total of 26,958 patients with NSCLC. Based on the lowest risk of any trAEs, cemiplimab, tislelizumab, and durvalumab were ranked as the best. Among the agents associated with the lowest risk of grades 3-5 trAEs, tislelizumab, avelumab, and nivolumab were most likely to rank highest. As far as any or grades 3-5 irAEs are concerned, atezolizumab plus bevacizumab plus chemotherapy is considered the most safety option. However, it is associated with a high risk of grades 3-5 trAEs. As a result of FAERS pharmacovigilance data analysis, 9,420 AEs cases have been identified in 7,339 NSCLC patients treated with ICIs, and ICIs were related to statistically significant positive signal with 311 preferred terms (PTs), and comprehensively investigated and identified those AEs highly associated with ICIs. In total, 152 significant signals were associated with Nivolumab, with malignant neoplasm progression, death, and hypothyroidism being the most frequent PTs.
Conclusion: These findings revealed that ICIs differed in their safety profile. ICI treatment strategies can be improved and preventive methods can be developed for NSCLC patients based on our results.
Keywords: FAERS; immune checkpoint inhibitors; non-small cell lung cancer; pharmacovigilance; real-world study.
Copyright © 2024 Liang, Xiao, Li, Chen and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials