

Unraveling the genetic basis of the causal association between inflammatory cytokines and osteonecrosis
- PMID: 38745949
- PMCID: PMC11091469
- DOI: 10.3389/fendo.2024.1344917
Unraveling the genetic basis of the causal association between inflammatory cytokines and osteonecrosis
Abstract
Background: Previous studies have reported that the occurrence and development of osteonecrosis is closely associated with immune-inflammatory responses. Mendelian randomization was performed to further assess the causal correlation between 41 inflammatory cytokines and osteonecrosis.
Methods: Two-sample Mendelian randomization utilized genetic variants for osteonecrosis from a large genome-wide association study (GWAS) with 606 cases and 209,575 controls of European ancestry. Another analysis included drug-induced osteonecrosis with 101 cases and 218,691 controls of European ancestry. Inflammatory cytokines were sourced from a GWAS abstract involving 8,293 healthy participants. The causal relationship between exposure and outcome was primarily explored using an inverse variance weighting approach. Multiple sensitivity analyses, including MR-Egger, weighted median, simple model, weighted model, and MR-PRESSO, were concurrently applied to bolster the final results.
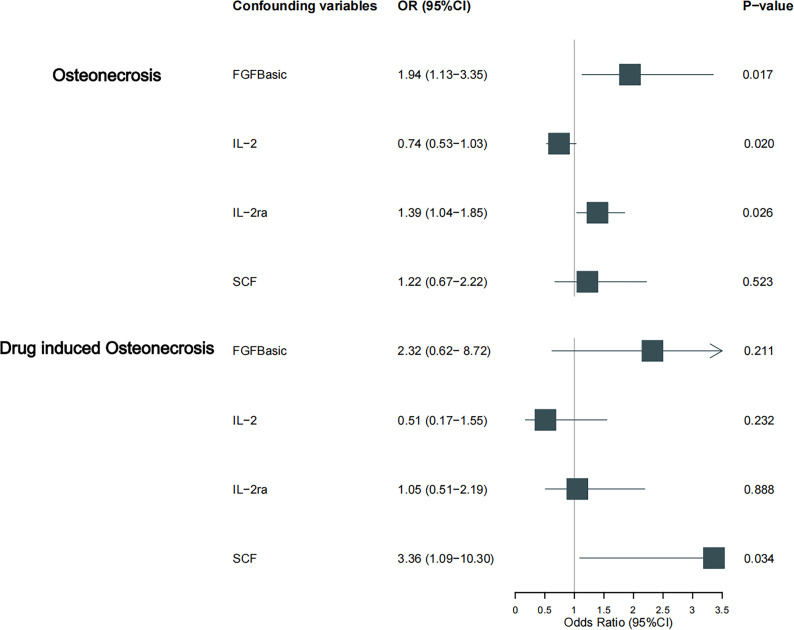
Results: The results showed that bFGF, IL-2 and IL2-RA were clinically causally associated with the risk of osteonecrosis (OR=1.942, 95% CI=1.13-3.35, p=0.017; OR=0.688, 95% CI=0.50-0.94, p=0.021; OR=1.386, 95% CI=1.04-1.85, p = 0.026). there was a causal relationship between SCF and drug-related osteonecrosis (OR=3.356, 95% CI=1.09-10.30, p=0.034).
Conclusion: This pioneering Mendelian randomization study is the first to explore the causal link between osteonecrosis and 41 inflammatory cytokines. It conclusively establishes a causal association between osteonecrosis and bFGF, IL-2, and IL-2RA. These findings offer valuable insights into osteonecrosis pathogenesis, paving the way for effective clinical management. The study suggests bFGF, IL-2, and IL-2RA as potential therapeutic targets for osteonecrosis treatment.
Keywords: GWAS; bone; immune; inflammation; mendelian randomization; necrosis.
Copyright © 2024 Lu, Pei, Gao, Zhao, Wang and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Jones JP., Jr. Coagulopathies and osteonecrosis. Acta orthopaedica Belgica. (1999) 65 Suppl 1:5–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical