

Microscopic Small Airway Abnormalities Identified in Early Idiopathic Pulmonary Fibrosis In Vivo Using Endobronchial Optical Coherence Tomography
- PMID: 38747674
- PMCID: PMC11351792
- DOI: 10.1164/rccm.202401-0249OC
Microscopic Small Airway Abnormalities Identified in Early Idiopathic Pulmonary Fibrosis In Vivo Using Endobronchial Optical Coherence Tomography
Abstract
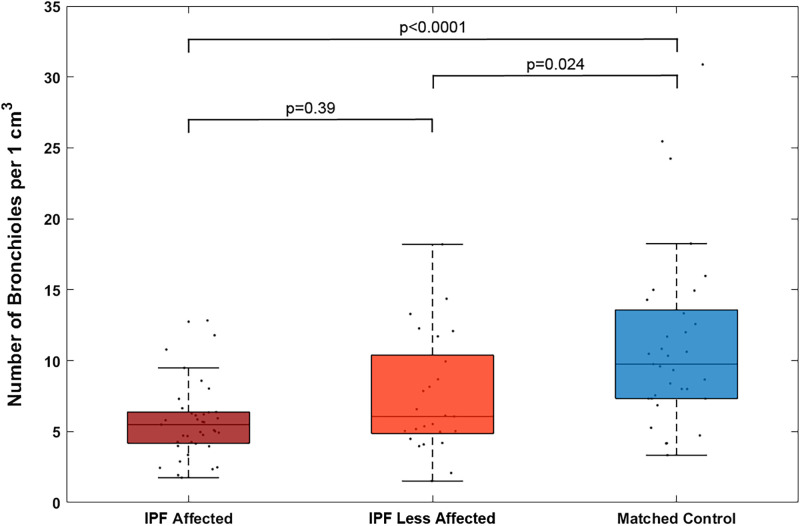
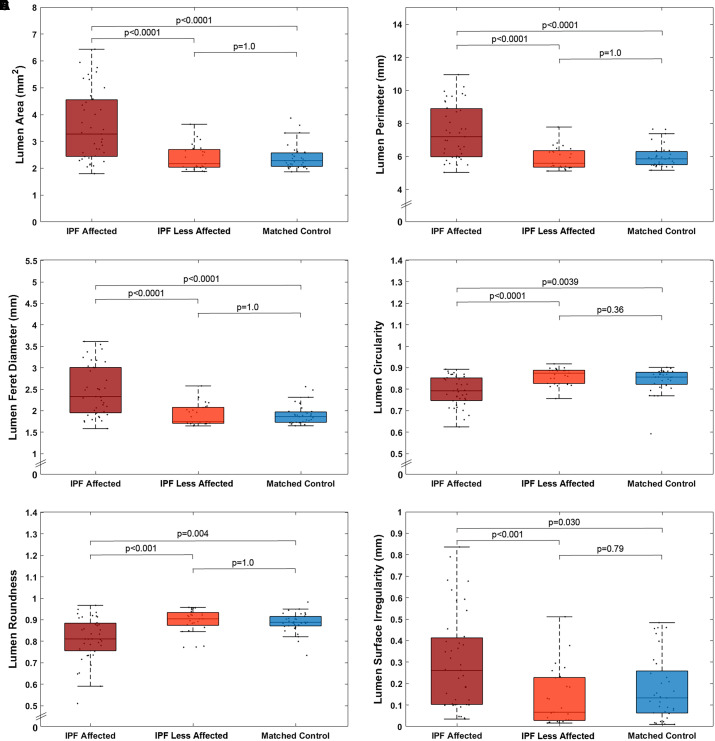
Rationale: Idiopathic pulmonary fibrosis (IPF) affects the subpleural lung but is considered to spare small airways. Micro-computed tomography (micro-CT) studies demonstrated small airway reduction in end-stage IPF explanted lungs, raising questions about small airway involvement in early-stage disease. Endobronchial optical coherence tomography (EB-OCT) is a volumetric imaging modality that detects microscopic features from subpleural to proximal airways. Objectives: In this study, EB-OCT was used to evaluate small airways in early IPF and control subjects in vivo. Methods: EB-OCT was performed in 12 subjects with IPF and 5 control subjects (matched by age, sex, smoking history, height, and body mass index). Subjects with IPF had early disease with mild restriction (FVC: 83.5% predicted), which was diagnosed per current guidelines and confirmed by surgical biopsy. EB-OCT volumetric imaging was acquired bronchoscopically in multiple, distinct, bilateral lung locations (total: 97 sites). IPF imaging sites were classified by severity into affected (all criteria for usual interstitial pneumonia present) and less affected (some but not all criteria for usual interstitial pneumonia present). Bronchiole count and small airway stereology metrics were measured for each EB-OCT imaging site. Measurements and Main Results: Compared with the number of bronchioles in control subjects (mean = 11.2/cm3; SD = 6.2), there was significant bronchiole reduction in subjects with IPF (42% loss; mean = 6.5/cm3; SD = 3.4; P = 0.0039), including in IPF affected (48% loss; mean: 5.8/cm3; SD: 2.8; P < 0.00001) and IPF less affected (33% loss; mean: 7.5/cm3; SD: 4.1; P = 0.024) sites. Stereology metrics showed that IPF-affected small airways were significantly larger, more distorted, and more irregular than in IPF-less affected sites and control subjects. IPF less affected and control airways were statistically indistinguishable for all stereology parameters (P = 0.36-1.0). Conclusions: EB-OCT demonstrated marked bronchiolar loss in early IPF (between 30% and 50%), even in areas minimally affected by disease, compared with matched control subjects. These findings support small airway disease as a feature of early IPF, providing novel insight into pathogenesis and potential therapeutic targets.
Keywords: idiopathic pulmonary fibrosis; interstitial lung disease; in vivo microscopy; small airways disease; usual interstitial pneumonia.
Figures


Comment in
-
Bystander No More: Small Airway Involvement in Idiopathic Pulmonary Fibrosis.Am J Respir Crit Care Med. 2024 Aug 15;210(4):383-385. doi: 10.1164/rccm.202405-1089ED. Am J Respir Crit Care Med. 2024. PMID: 38980193 Free PMC article. No abstract available.
References
-
- Katzenstein AL, Mukhopadhyay S, Myers JL. Diagnosis of usual interstitial pneumonia and distinction from other fibrosing interstitial lung diseases. Hum Pathol . 2008;39:1275–1294. - PubMed
-
- Larsen BT. Usual interstitial pneumonia: a clinically significant pattern, but not the final word. Mod Pathol . 2022;35:589–593. - PubMed
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, et al. ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med . 2011;183:788–824. - PMC - PubMed
-
- Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, et al. American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med . 2018;198:e44–e68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
