

Evaluating the efficacy of laparoscopic radical antegrade modular pancreatosplenectomy in selected early-stage left-sided pancreatic cancer: a propensity score matching study
- PMID: 38750173
- PMCID: PMC11219433
- DOI: 10.1007/s00464-024-10868-x
Evaluating the efficacy of laparoscopic radical antegrade modular pancreatosplenectomy in selected early-stage left-sided pancreatic cancer: a propensity score matching study
Abstract
Background: Laparoscopic radical pancreatectomy is safe and beneficial for recectable pancreatic cancer, but the extent of resection for early-stage tumors remains controversial.
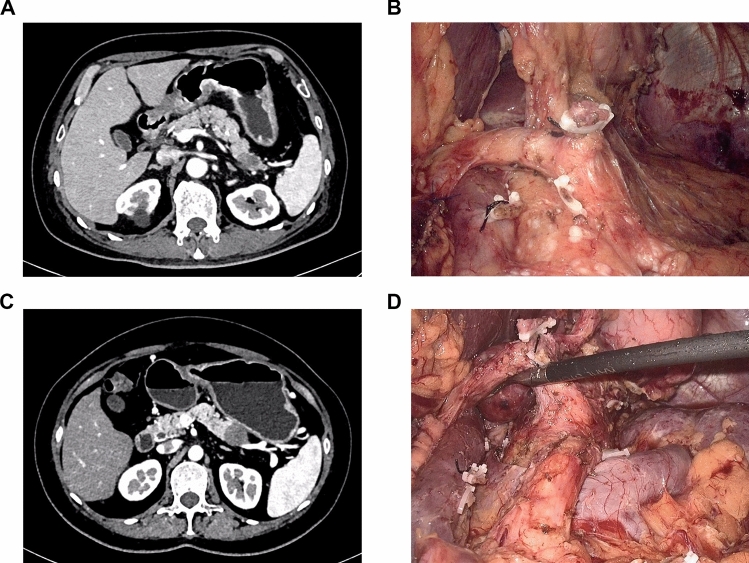
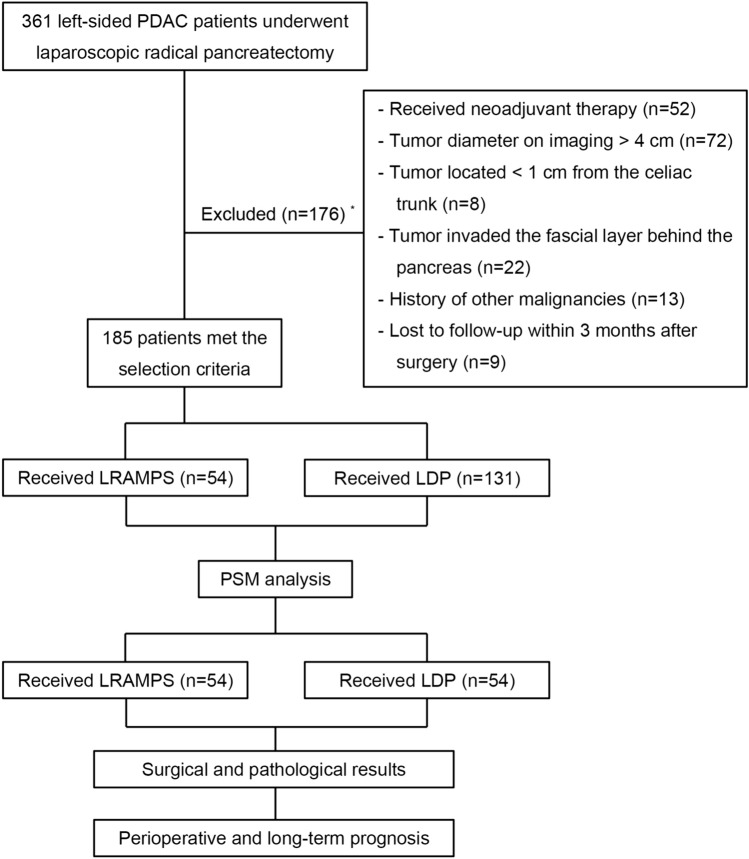
Methods: Consecutive patients with left-sided pancreatic cancer who underwent either laparoscopic radical antegrade modular pancreatosplenectomy (LRAMPS, n = 54) or laparoscopic distal pancreatosplecnectomy (LDP, n = 131) between October 2020 and December 2022 were reviewed. The preoperative radiological selection criteria were as follows: (1) tumor diameter ≤ 4 cm; (2) located ≥ 1 cm from the celiac trunk; (3) didn't invade the fascial layer behind the pancreas.
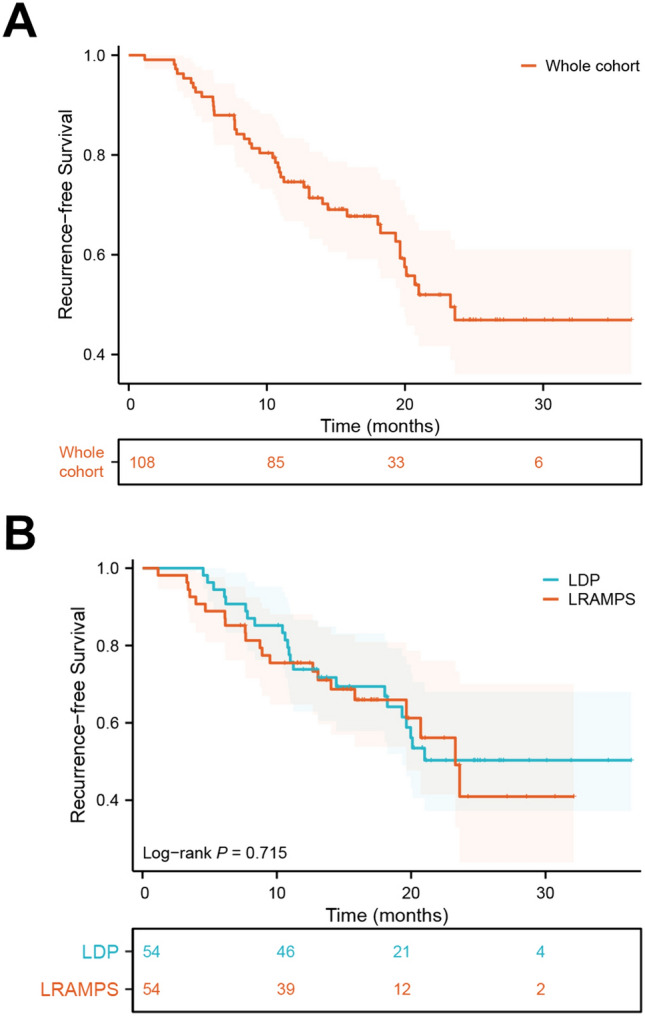
Results: After 1:1 propensity score matching (LRAMPS, n = 54; LDP, n = 54), baseline data were well-balanced with no differences. LRAMPS resulted in longer operation time (240.5 vs. 219.0 min, P = 0.020) and higher intraoperative bleeding volume (200 vs. 150 mL, P = 0.001) compared to LDP. Although LRAMPS harvested more lymph nodes (16 vs. 13, P = 0.008), there were no statistically significant differences in lymph node positivity rate (35.2% vs. 33.3%), R0 pancreatic transection margin (94.4% vs. 96.3%), and retroperitoneal margin (83.3% vs. 87.0%) rate. Postoperative complications did not significantly differ between the two groups. However, LRAMPS was associated with increased drainage volume (85.0 vs. 40.0 mL, P = 0.001), longer time to recover semi-liquid diet compared to LDP (5 vs. 4 days, P < 0.001) and increased daily bowel movement frequency. Tumor recurrence pattern and recurrence-free survival were comparable between the two groups, but the adjuvant chemotherapy regimens varied, and the completion rate of the 6-month intravenous chemotherapy was lower in the LRAMPS group compared to the LDP group (51.9% vs. 75.9%, P = 0.016).
Conclusions: LRAMPS did not provide oncological benefits over LDP for left-sided pancreatic cancer within the selection criteria, but it increased operation time, intraoperative bleeding, and postoperative bowel movement frequency. These factors impacted the regimen selection and completion of adjuvant chemotherapy, consequently compromising the potential benefits of LRAMPS in achieving better local control.
Keywords: Early-stage tumor; Laparoscopic distal pancreatosplecnectomy; Laparoscopic radical antegrade modular pancreatosplenectomy; Left-sided pancreatic cancer; Oncologic prognosis; Surgical complication.
© 2024. The Author(s).
Conflict of interest statement
Zheng Li, Wenyan Xu, Ting Wang, Borui Li, Chen Chen, Yihua Shi, Chenjie Zhou, Qifeng Zhuo, Shunrong Ji, Wensheng Liu, Xianjun Yu, Xiaowu Xu have no conflicts of interest or financial ties to disclose.
Figures
Similar articles
-
Comparison of Radical Antegrade Modular Pancreatosplenectomy Versus Standard Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma: A Propensity Score Matching Study.World J Surg. 2025 Jul;49(7):1870-1880. doi: 10.1002/wjs.12630. Epub 2025 Jun 18. World J Surg. 2025. PMID: 40533171
-
Laparoscopic radical antegrade modular pancreatosplenectomy: preliminary experience with 10 cases.BMC Surg. 2021 Feb 10;21(1):78. doi: 10.1186/s12893-021-01090-w. BMC Surg. 2021. PMID: 33568109 Free PMC article.
-
Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: a systematic review and meta-analysis.Ann Surg. 2012 Jun;255(6):1048-59. doi: 10.1097/SLA.0b013e318251ee09. Ann Surg. 2012. PMID: 22511003
-
Comparison of laparoscopic versus open radical antegrade modular pancreatosplenectomy for pancreatic cancer: A systematic review and meta-analysis.Int J Surg. 2022 Jul;103:106676. doi: 10.1016/j.ijsu.2022.106676. Epub 2022 May 13. Int J Surg. 2022. PMID: 35577311
-
Radical antegrade modular pancreatosplenectomy versus standard procedure in the treatment of left-sided pancreatic cancer: A systemic review and meta-analysis.BMC Surg. 2017 Jun 5;17(1):67. doi: 10.1186/s12893-017-0259-1. BMC Surg. 2017. PMID: 28583142 Free PMC article.
Cited by
-
Laparoscopic radical antegrade modular pancreatosplenectomy vesus laparoscopic distal pancreatosplenectomy for left-sided pancreatic cancer: a systematic review and meta-analysis.Front Oncol. 2025 Feb 14;15:1510342. doi: 10.3389/fonc.2025.1510342. eCollection 2025. Front Oncol. 2025. PMID: 40027121 Free PMC article.
References
-
- Korrel M, Jones LR, van Hilst J, Balzano G, Björnsson B, Boggi U, et al. Minimally invasive versus open distal pancreatectomy for resectable pancreatic cancer (DIPLOMA): an international randomised non-inferiority trial. Lancet Reg Health Eur. 2023;31:100673 . doi: 10.1016/j.lanepe.2023.100673. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- 20224Z0006/Excellence Project of Shanghai Municipal Health Commission
- 22YF1409000/Sailing Project of Science and Technology Commission of Shanghai Municipality
- 20234Y0119/Clinical Research Project of Health Industry of Shanghai Municipal Health Commission
- 21JC1401500/Shanghai Municipal Science and Technology Major Project
- 2019-01-07-00-07-E00057/Scientific Innovation Project of Shanghai Education Committee
LinkOut - more resources
Full Text Sources
Medical
