

Statins did not reduce the frequency of exacerbations in individuals with COPD and cardiovascular comorbidities in the COSYCONET cohort
- PMID: 38750572
- PMCID: PMC11097413
- DOI: 10.1186/s12931-024-02822-1
Statins did not reduce the frequency of exacerbations in individuals with COPD and cardiovascular comorbidities in the COSYCONET cohort
Abstract
Background: The evidence regarding effects of statins on exacerbation risk in COPD remains controversial. Previous studies often excluded patients with cardiovascular comorbidities despite their high prevalence in COPD and role for exacerbations. Based on the cardioprotective properties of statins, we hypothesised that statins may reduce the risk of exacerbations especially in patients with cardiovascular comorbidities.
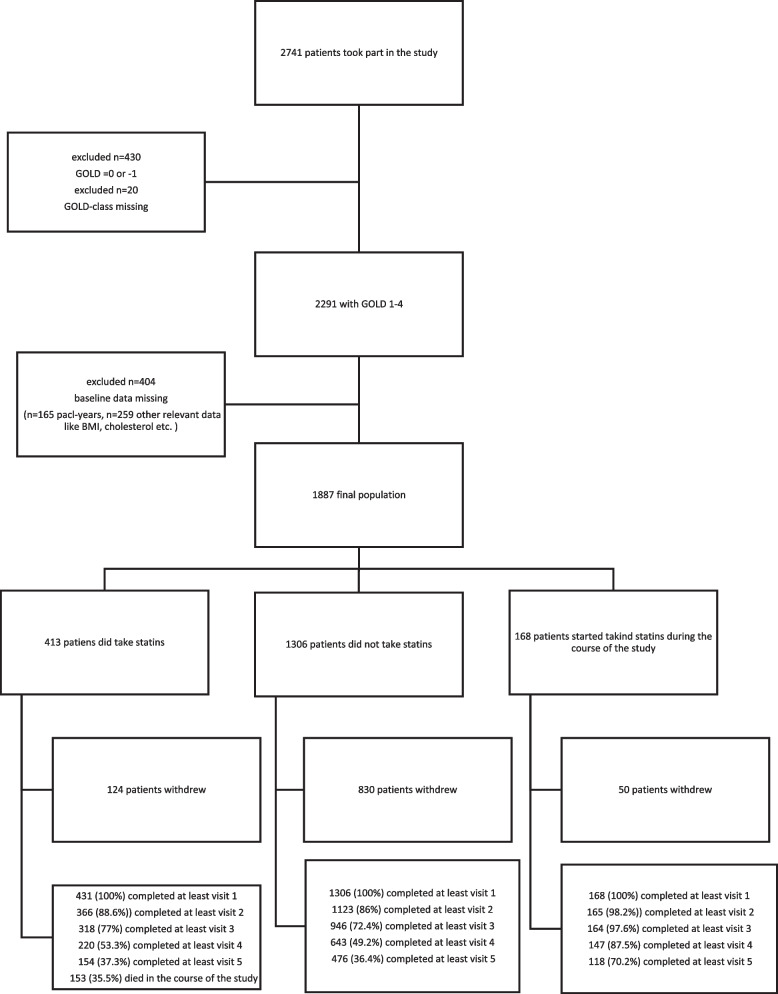
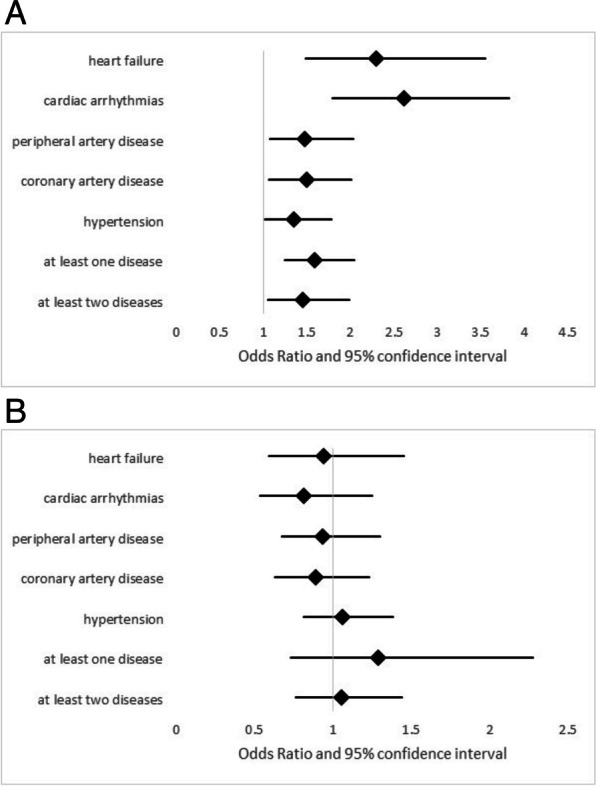
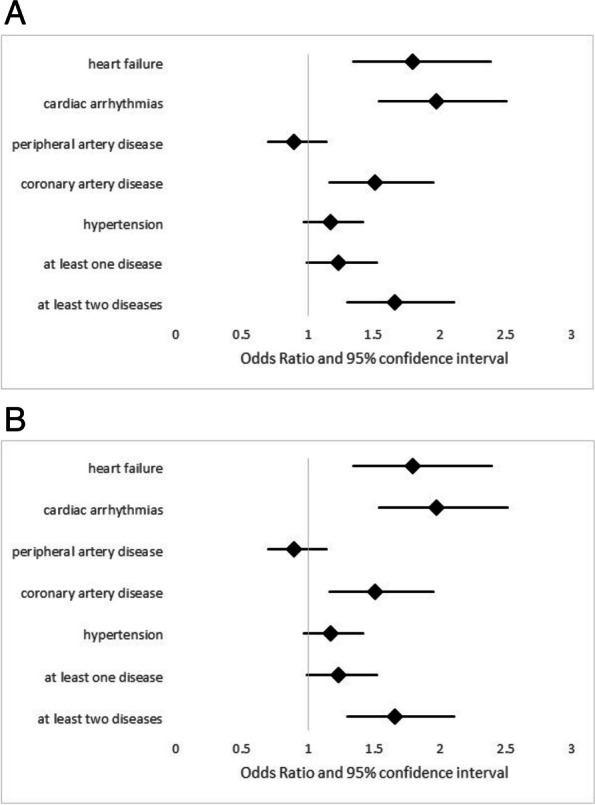
Methods: One thousand eight hundred eighty seven patients of the German COPD cohort COSYCONET (COPD and Systemic Consequences Comorbidities Network) of GOLD grades 1-4 (37.8% female, mean age 64.78 ± 8.3) were examined at baseline and over a period of 4.5 years for the occurrence of at least one exacerbation or severe exacerbation per year in cross-sectional and longitudinal analyses adjusted for age, gender, BMI, GOLD grade and pack-years. Due to their collinearity, various cardiovascular diseases were tested in separate analyses, whereby the potential effect of statins in the presence of a specific comorbidity was tested as interaction between statins and comorbidity. We also identified patients who never took statins, always took statins, or initiated statin intake during the follow-up.
Results: One thousand three hundred six patients never took statins, 31.6% were statin user, and 12.9% initiated statins during the follow-up. Most cardiovascular diseases were significantly (p < 0.05)may associated with an increased risk of COPD exacerbations, but in none of them the intake of statins was a significant attenuating factor, neither overall nor in modulating the increased risk linked to the specific comorbidities. The results of the cross-sectional and longitudinal analyses were consistent with each other, also those regarding at least 1 exacerbation or at least 1 severe exacerbation per year.
Conclusion: These findings complement the existing literature and may suggest that even in patients with COPD, cardiovascular comorbidities and a statin therapy that targets these comorbidities, the effects of statins on exacerbation risk are either negligible or more subtle than a reduction in exacerbation frequency.
Trial registration: Trial registration ClinicalTrials.gov, Identifier: NCT01245933. Other Study ID (BMBF grant): 01GI0881, registered 18 November 2010, study start 2010-11, primary completion 2013-12, study completion 2023-09. https://clinicaltrials.gov/study/NCT01245933?cond=COPD&term=COSYCONET&rank=3.
Keywords: COPD; Cardiovascular comorbidities; Exacerbations; Statins.
© 2024. The Author(s).
Conflict of interest statement
Robert Bals is a member of the Editorial Board at Respiratory Research.
Figures

References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–82. doi: 10.1164/rccm.201701-0218PP. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
- number 01 GI 0881/Bundesministerium für Bildung und Forschung
LinkOut - more resources
Full Text Sources
Medical
